In this study, we evaluated the utility of %CDT measurement in an Asian population with NAFLD or ALD and comorbid MetS-related factors. The male:female ratio was approximately equal in the non-drinker group; in contrast, the majority of patients were men in the other groups. The heavy-drinker group had higher HDL and lower BMI values, which are consistent with the general characteristics of patients with ALD (Table 1). Because even a relatively small amount of alcohol can cause liver injury in patients with obesity and/or MetS [8], Obtaining detailed quantitative information on alcohol intake is vital in the medical care of patients with fatty liver disease. Our cohort included more than half of participants with light or moderate drinking levels, in contrast to previous studies on %CDT involving patients with alcohol addiction [17–19]; thereby enabling the investigation on the usefulness of %CDT in patients with light-to-moderate alcohol intake.
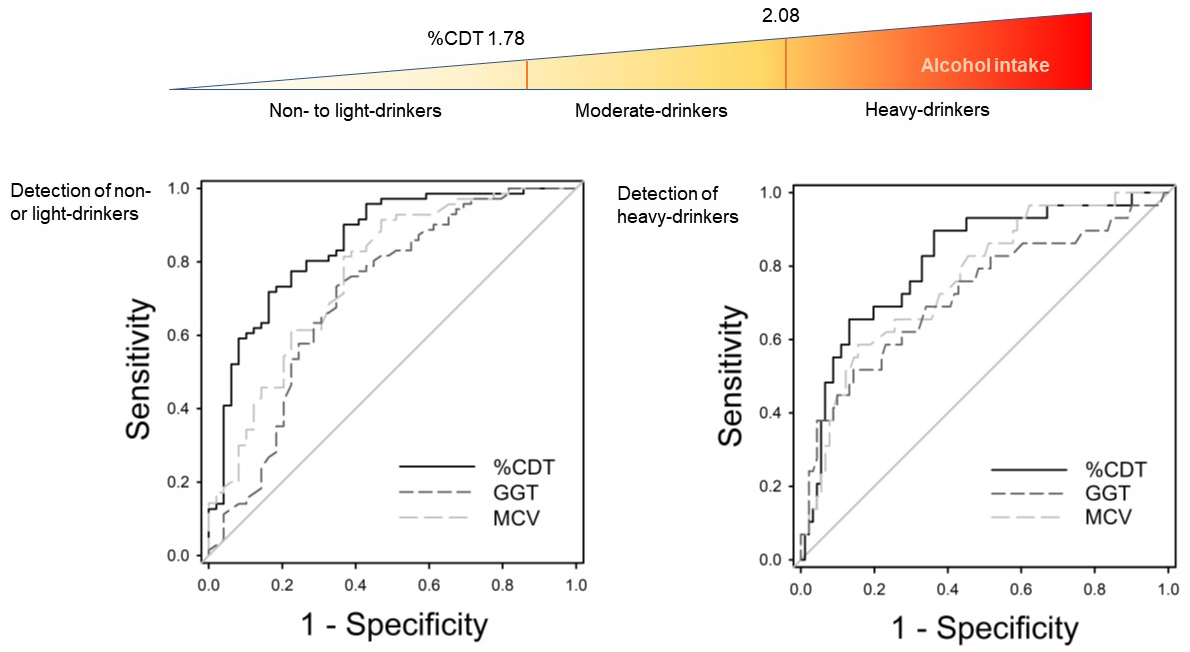
This study showed that %CDT had higher AUROCs than either GGT or MCV, indicating good diagnostic accuracy for distinguishing the absence of significant drinking (< 210 g/week for men, < 140 g/week for women), which is an important diagnostic criterion for NAFLD, from the presence of heavy drinking (> 420 g/week), which is a diagnostic criterion for ALD. Particularly, the %CDT showed a significantly higher AUROC than GGT for identifying a lack of significant drinking (Fig. 1).
To our knowledge, our study, which was conducted on a cohort in which the majority of patients exhibited light-to-moderate drinking levels, was the first to show that %CDT is more useful than GGT or MCV for determining the presence or absence of drinking using the diagnostic criteria for NAFLD and ALD. A %CDT cut-off value of 1.78% was used to identify non- or light drinkers, and a cut-off value of 2.08% was used to identify heavy drinkers. These values showed high sensitivities of 71.8% and 65.5%, respectively, and excellent specificities of 83.7% and 86.8%, respectively. Indeed, in the moderate- to heavy- drinker groups, 10 of 14 patients had low GGT levels that were less than the upper limit of normal (ULN, 75 U/L). These patients were considered GGT non-responders, with excessive drinking identified by a %CDT value exceeding the ≥ 1.78% cut-off. By contrast, 20 of the 29 non-to-light drinkers had GGT values more than the ULN but a %CDT of < 1.78%. Similarly, 25 out of 33 moderate- to heavy-drinkers with MCVs less than the ULN (99.0 fl) showed a %CDT of ≥ 1.78%, whereas 1 out of 3 non- to light-drinkers with MCVs higher than the ULN showed a %CDT of < 1.78% (data not shown). These findings indicate that %CDT can be used to correctly identify non-light drinkers, even in patients with misleading GGT or MCV values.
Although several studies have shown that the %CDT is an excellent alcohol marker for detecting heavy drinkers, most of these studies were conducted in extreme cohorts of heavy drinkers or those practicing abstinence. A clinical study in Germany showed that the %CDT was more specific than either GGT or MCV for distinguishing ALD due to current alcohol dependence form liver damage due to other causes (mostly viral hepatitis) [18]. A Finnish study reported that the %CDT was more sensitive than GGT or MCV for distinguishing alcohol abusers from healthy volunteers who were either abstainers or moderate drinkers [20]. In Asia, Liang et al. reported that the %CDT was a better indicator than either GGT or MCV for distinguishing an alcoholic group from healthy controls or a non-alcoholic liver disease group in China [21], while Suzuki T et al. showed that the %CDT was a more useful biomarker of chronic alcohol abuse than GGT during treatment of patients with alcoholism in Japan [19].
Serum markers that can identify insignificant alcohol intake for the diagnosis of NAFLD have not yet been established. In this study of 120 Japanese patients, the AUROC of the %CDT was greater for detecting non- or light drinkers than heavy drinkers (Fig. 1), and the %CDT value was significantly elevated with only minimal increases in daily drinking from 0–2 drinks to 3–4, indicating a sharp increase with a small EtOH increase of only 20 g/day (Table 2). Therefore, the %CDT level appears to be very helpful for identifying heavy drinkers and distinguishing non- or light drinkers from moderate drinkers. A threshold effect on manufacturer-recommended CDT value of 2.6% in healthy subjects with an alcohol intake of over 40 g per day was reported in France [22]. Thus, racial differences in %CDT values may need to be considered in the discrimination of insignificant drinkers. Regarding drinking frequency, the %CDT did not significantly increase until the frequency was as high as four or more times per week. Similarly, even with heavy drinking of six drinks or more at a time, the %CDT did not significantly increase unless the frequency was as high as “almost daily.” Thus, using an elevated %CDT to evaluate alcohol consumption did not require clinically significant daily doses but only frequent drinking.
Candidate factors that could potentially influence drinking markers, including serum AST and ALT levels; hepatic steatosis by CAP values; hepatic elasticity by LSM; BMI; and other MetS-related factors such as HDL, LDL, TG, hypertension, and HbA1c were evaluated in this study. To evaluate these factors, the study cohort was divided into two groups depending on whether each factor was within its respective threshold, and two-group comparisons of drinking markers were performed (Table 3). The GGT value fluctuated depending on whether the AST and ALT values were less than the ULN, suggesting that liver damage can affect GGT. The MCV was significantly lower with high LDL levels, indicating it may be affected by lipid metabolism. The %CDT was low in the high-BMI group, consistent with previous studies reporting that high-BMI groups are less likely to have an increased %CDT than low-BMI groups [23, 24]; however, the detailed mechanisms underlying this phenomenon remain unknown [23].
A simple linear regression analysis (Table 4), followed by a multiple linear regression analysis (Table 5), demonstrated that a low BMI independently affected the increase in %CDT, while many other factors did not affect it. By contrast, GGT was independently influenced by various factors, including the AST, liver stiffness, and TG. MCV increased the p-value associated with alcohol intake to the limit of significance, suggesting that MCV is also influenced by many background factors. MCV was independently affected by several factors, including the AST, HDL, LDL, and HbA1c. Taken together, the %CDT value was found to be an almost-pure drinking marker, whereas GGT and MCV values reflected not only the amount of drinking, but also liver damage and disorders of lipid metabolism.
In 2020, the European Association for the Study of the Liver proposed metabolic dysfunction-associated fatty disease (MAFLD) as a new pathological concept, indicating that fatty liver disease can be associated with metabolic disorders.[25] This major shift in the field of liver disease suggests that fatty liver disease will be regarded as a series of liver diseases centered on dyslipidemia, with drinking being a major factor. Therefore, it is expected that using %CDT, a drinking marker not affected by liver damage or dyslipidemia, to objectively analyze a predominant factor underlying the pathogenesis of these disorders and determine a treatment policy for patients with MAFLD will become vitally important.
In conclusion, this study showed that the %CDT is a highly useful drinking marker for diagnosing NAFLD and ALD. While a low BMI could affect %CDT, the %CDT was not influenced by liver damage or lipid metabolism disorders, unlike the MCV or GGT, indicating that this parameter can be used to identify fatty liver disease associated with NAFLD and ALD comorbid with MetS, which is currently the predominant form of liver disease and is expected to account for a higher proportion of patients in the future.
{kind=link}