In this study, we described HCC risk in alcoholic liver cirrhosis, and developed a risk stratification model for HCC (i.e., ALICE score) in a hospital-based cohort. Unlike the recently developed prediction models [14, 15], we employed competing-risk analysis by incorporating mortality data from causes other than HCC. Liver cirrhosis is typically a multistate disease complicated by discrete outcomes [28]. If patients with competing outcomes such as non-HCC deaths are simply treated as right-censored cases, Kaplan Meier method may overestimate the real cumulative risks [28, 29]. Moreover, the predicted risk of HCC does not necessarily correlate with the predicted rate by Cox model of HCC prediction [29]. Our cohort patients showed that censored cases due to non-HCC deaths were twice more than those censored due to HCC.
The estimated cumulative HCC risk in our cohort was ~ 1.5 % per year for overall patients (Fig. 1), and approximately 1.0 % for patients without markers of viral hepatis. The latter figure fell in the range between the two recent European studies (0.7 [10] and 1.8 % [9]) which excluded patients with chronic viral hepatitis. Comorbid viral hepatitis is of special interest in geographic areas whe re chronic hepatitis virus infection is prevalent. Interestingly, our cohort showed higher prevalence of chronic viral hepatitis compared to Korean general population: 2.9 % for HBV [19] and ~ 0.8 % for HCV [30]. This high prevalence may be explained by the synergistic effect of comorbid viral hepatitis on the accelerated progression of alcoholic fatty liver to alcoholic cirrhosis [31].
The role of HCC surveillance in alcoholic liver disease is still under debate. Practice guidelines recommend HCC surveillance in patients with cirrhosis due to alcohol and other etiologies on the ground that threshold HCC incidence of > 1.5 %/year may justify cost-effectiveness of surveillance [3, 23, 32]. However, not only the “1.5 %/year” cut-off itself has been doubted [33], but also the risk of HCC in alcoholic cirrhosis may not be high enough to ensure cost-effectiveness [5, 10]. Risk stratification may be thus necessary to enhance the effectiveness of HCC surveillance in alcoholic cirrhosis.
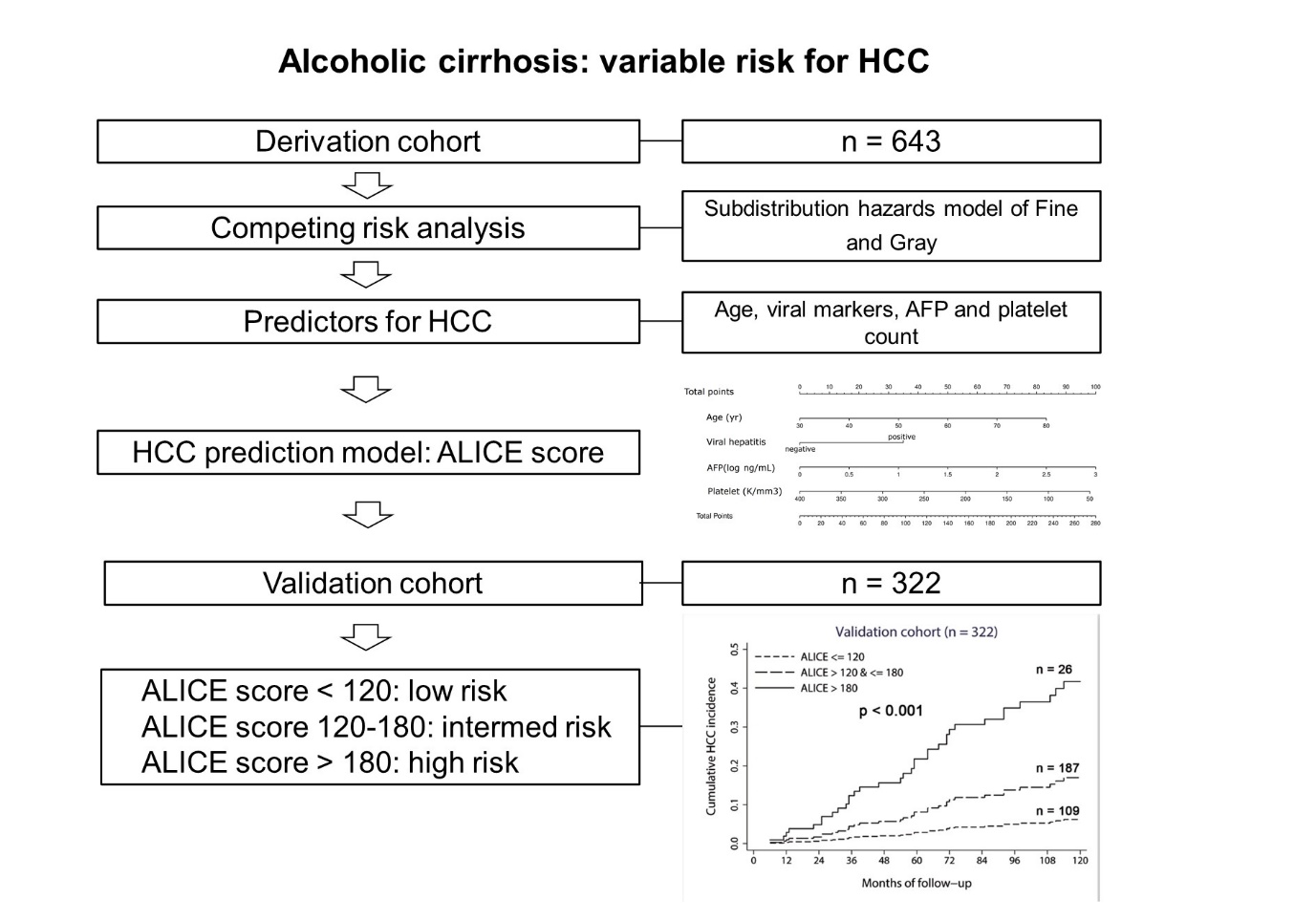
We have built our risk stratification model based on four independent predictors of HCC risk: age, chronic viral hepatitis, AFP level, and platelet count. AFP level was a significant predictor in addition to other well-established markers [14, 15], and this finding is in concordance with the French cohort study [9]. These four factors are readily available in routine practice, and nomogram-based ALICE score was able to discriminate the low, high, and super high-HCC risk groups in alcoholic cirrhosis. Patients with ALICE score ≤ 120 carries minimal risk for HCC and may not be indicated for routine HCC surveillance, whereas those with ≥180 show highest risk for HCC and regular surveillance may be justified. In other word, the ALICE score may serve dual purposes: (1) to exclude ALD patients with low risk from HCC surveillance, and (2) to identify patients with very high risk for HCC in need of enhanced surveillance. Further studies will be necessary to assess whether risk-based surveillance is cost-effective in alcoholic cirrhosis.
Recently, a HCC risk stratification model was developed from US Veterans Affairs healthcare system (VAHS) data including a large number of alcoholic cirrhosis (n = 16,175) [15]. The model was based on 8 parameters and the score is available through a web-based calculator. As mentioned above, competing risks were not considered in the US-VA model building. Moreover, a significant fraction of alcoholic cirrhosis with viral markers will not be properly assessed by the US-VA model. Time-dependent ROC analysis showed that the ALICE score had comparable or higher AUC values compared with the US-VA score (Fig. 4). Compared to the US-VA model, our score is more parsimonious with using only 4 readily available parameters. However, further validation would be warranted for the clinical utility of ALICE score by prospective studies.
There are potential limitations in our study, mainly related to the retrospective design in a limited number of institutions. We tried to minimize selection bias by using our pre-defined EMR system[20, 34] and validated the model in an internal validation cohort; however, further external validation is needed by prospective studies. Cost-effectiveness analysis should also be conducted for the clinical utility of ALICE score-guided surveillance strategy. Finally, the diagnosis of cirrhosis was mostly made clinically, and there was a possibility that liver cirrhosis was underdiagnosed and not included in our cohort [35, 36]. Since liver biopsy is not generally required for the management of compensated alcoholic liver disease, however, we believe that our model can be applicable to real-world practice of clinically diagnosed alcoholic liver cirrhosis.
In conclusion, a novel HCC risk score, the ALICE score, which includes age, chronic viral hepatitis, AFP level, and platelet count, represents a reliable and easy-to-use method for predicting HCC development in patients with alcoholic cirrhosis in areas where the prevalence of viral hepatitis is substantial.
{kind=link}