Patients
The study project and the protocols were approved by the Ethics Committee of the Changzhou maternal and child health care hospital. The sighed informed consent was obtained from all patients. All the data in the study were collected from patients undergoing standard and routine IVF treatment.
Data (2698 cycles) in the retrospective analysis were collected from IVF cycles with a GnRH antagonist or agonist pituitary suppression protocol (GnRHa long Protocol and Ultra-long Protocol), that were performed in the IVF Unit of Changzhou maternal and child health care hospital in 2017–2019. Exlcusion criteria:(1)patient with chromosomal abnormal on either side of the couple;(2)Patients with ovarian cysts at the start of the ovarian stimulation procedure;(3)Patients with abnormal uterine cavity, ovarian deficiency and other organic disease; The fresh embryo transfer (ET) was cancelled in the case of increasing progesterone levels (p ≥ 1.0ng/ml).
Ovarian stimulation
Three protocols for controlled ovarian stimulation were performed based on age, anti-üllerian hormone (AMH) levels, number of antral follicles (AFC) and previous ovarian response, either recombinant FSH (Gonal F, Merck Serono, Geneva, Switzerland) or human menopausal gonadotrophin (HMG; 75 IU; Livzon Pharmaceutical, China) was used with daily doses between 150 and 300 IU. In the agonist long group, 0.1mg triptorelin (Decapeptyl, Ipsen, Paris, France) was administered for 7 days on menstrual cycle day 3 for inhibition of pituitary. In the ultra-long group, a long-acting gonadotrophin-releasing agonist (leuprorelin acetate, 3.75 mg, Lizhu Pharmaceutical Trading Co.) was administered on the menstrual cycle day 3 for pituitary inhibition. In the antagonist group, FSH/HMG was started on cycle day 3 and 0.25 cetrorelix (Cetrotide®, Merck Serono, Geneva, Switzerland) was injected subcutaneously as a daily dose from the 6th day of stimulation until the day of oocyte maturation triggering. Adjustment of FSH/HMG dose was performed according to the ovarian response as assessed by ultrasonography and serum estradiol levels. When ≥ 3 follicles in a mean diameters of ≥ 18mm were present, HCG(5000IU urinary HCG and 250ug recombinant HCG) were administered to trigger final oocyte maturation. Oocyte retrieval was performed approximately 35h-37h later.
In vitro fertilization and embryo culture
Depending on the semen parameters, fertilization of the retrieved oocyte was performed in vitro by either conventional IVF or ICSI. Cleavage embryo was assessed for number and regularity of blastomeres and the degree of embryonic fragmentation; Grade I and Grade II embryos were top-quality embryos, the criteria were described previous.[12] Blastocyst embryo was evaluated for expansion degree and the number of inner cell mass and trophoblast cells on the basis of Garden scoring method. [13]
If the patient conditions were allowed, one good-quality blastocyst embryo on day 5(6) was selected for transfer.
Hormonal analysis
Serums sample were collected on the moring of menstrual cycle day 3 and the day of HCG trigger during ovarian stimulation. Serum FSH, LH, E2, and progesterone levels were measured routinely by commercially available kits (Abbott Biologicals B.V. The Netherlands) based on chemiluminescence. The lower limits of sensitivity were as follows: FSH = 0.06 mIU/ml, LH = 0.09 mIU/ml, E2 = 10 pg/ml and P = 0.1 ng/ml. Intra- and interassay precision rates at the concentrations, expressed as coefficients of variance were 3.8% and 6.4% for LH, 21.0% and 12.0% for E2 and 9.57% and 11.19% for progesterone respectively.
PE definition
Previously, it had been demonstrated that serum progesterone levels elevation on the day of hCG administration were associated with reduced ongoing pregnancy rates. Although most of the studies presented that progesterone’s cut-off point for PE is 1.5ng/ml, a meta-analysis including several thousand fresh IVF-ET cycles, observed a detrimental effect on pregnancy rates when the progesterone levels exceed 0.9ng/ml on the HCG trigger day[11]. Present study also confirmed that the clinical pregnancy rate significantly decreased as soon as progesterone levels exceed 0.9ng/ml(60.26 & 50.56, P<0.05).For the above reason, PE occurrence was defined as progesterone ≥ 0.9 ng/mL. The population was divided into two groups: No PE group and PE group.
Statistical analysis
Two independent sample t-test, Nonparametric tests, and the Chi-squared test were performed to explore the distribution of baseline characteristics (ages, BMI, years of infertility et al.) and basal (day 3) hormonal profile between the two groups, and to predict the occurrence of PE after ovarian stimulation.
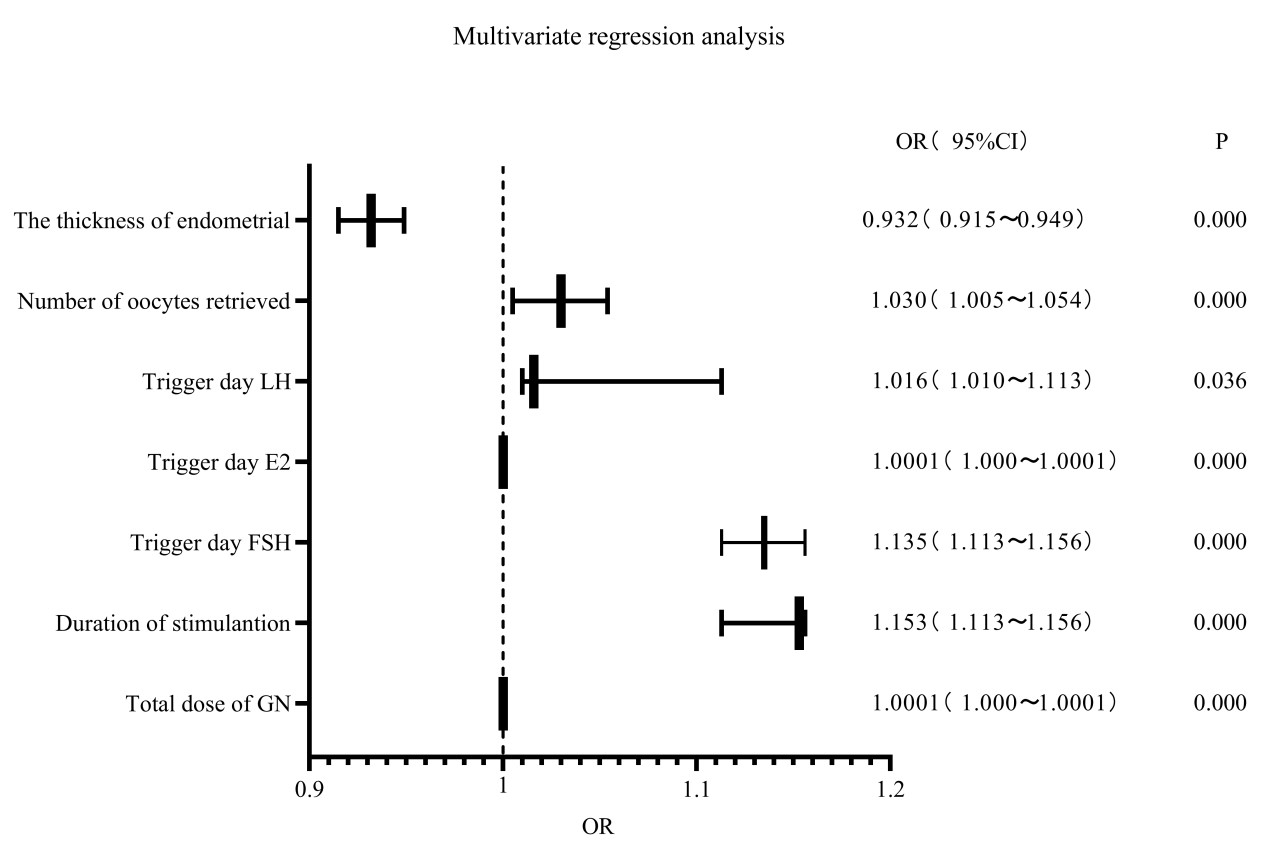
Logistic regression was performed to explore the multivariate model and to predict PE occurrence, and the regression models, the odds ratio (OR) and 95% Confidence Intervals (CI) were estimated. Multivariate logistic regression analysis was used to generate coefficients for each variable and the constant in the equation. The predictive accuracy of the models was measured using the average optimism of the area under the curve (AUC), quantifying the level of agreement between the predicted probabilities and the actual possibility of having the event of interest. A Nomogram was constructed to be a graphic representation of the prediction model with the R software. Hosmer and Leme test checked for calibration and differentiation.
Data analysis was done with Statistical Package for Social Sciences (SPSS) version 26.0 (SPSS Incl., USA). The significance level for all statistical tests was P ≤ 0.05.
{kind=link}