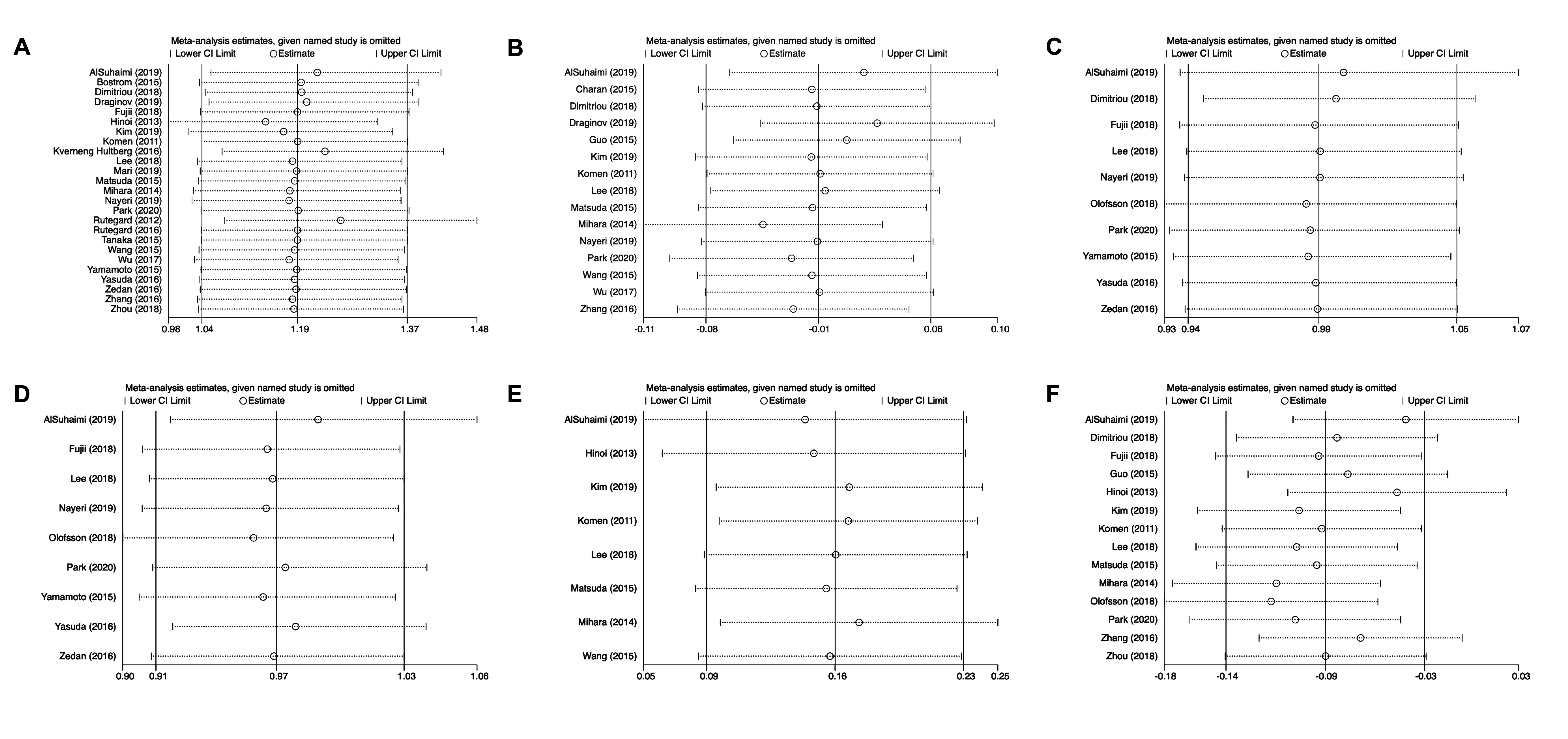
In this meta-analysis, long-term outcomes of interest were generally comparable between LCA preservation and non-preservation in CRC surgery. The pooled results revealed that the rate of anastomotic leakage after LCA preservation surgery was slightly lower than that after non-preservation surgery. However, this difference became statistically insignificant in the pooled result of the subgroup analysis of RC alone. Moreover, LCA non-preservation surgery could dissect more metastatic lymph nodes than the LCA preservation surgery. The operative time was significantly shorter in LCA non-preservation surgery than in LCA preservation surgery.
Although some excellent meta-analyses have been published in the past few years, the optimal procedure for CRC in handling the LCA remains controversial [8–13]. To our knowledge, no published meta-analysis has compared the preservation and non-preservation of the LCA in RC alone. Therefore, we summarized previously reported data including more recently published and high-quality studies (especially RCTs), and to identify the optimal procedure for CRC, we compared the oncological and perioperative outcomes between LCA preservation and non-preservation in the surgical treatment of CRC and RC.
Anastomotic leakage is the most devastating complication in CRC surgery and one of the most important reasons why the optimization of the procedure in CRC is drawing so much attention. The reported postoperative occurrence risk is 2.2%-12% [47], despite the advancements in laparoscopic techniques and the well-accepted concept of total mesocolic excision. The blood supply and tension of the anastomosis are two major factors affecting the rate of anastomotic leakage [48]. In our opinion, for cancers located in the descending colon or the sigmoid colon, the ligation of the sigmoid artery and superior rectal artery would greatly compromise blood supply of the bowel distal to the anastomosis stoma. Meanwhile, blood supply from the pudendal artery system to the lengthy rectal stump is limited. Therefore, blood perfusion becomes a more important factor that could influence the healing of the anastomosis stoma. In RC, the rectal stump distal to the anastomosis stoma could be well perfused by blood supply from underneath. In this case, the relatively lower position of the anastomosis stoma may make the tension of the intestine a more dominant factor of anastomosis [49]. The conservation of the LCA would decrease the mobility of the proximal intestine by approximately 6–9 cm, which could increase the tension of the anastomotic stoma [50, 51], and this may balance out the benefit of better blood supply. Besides, a protective stoma of the distal ileum was more common in radical surgery for mid-low RC, which would also influence the diagnosis of anastomosis leakage [52]. To our knowledge, the balance between better perfusion provided by LCA preservation and the less tension of the colon limb proximal to the anastomotic stoma with LCA ligation should be determined by the location of the cancer and be evaluated according to the intraoperative circumstance of each case.
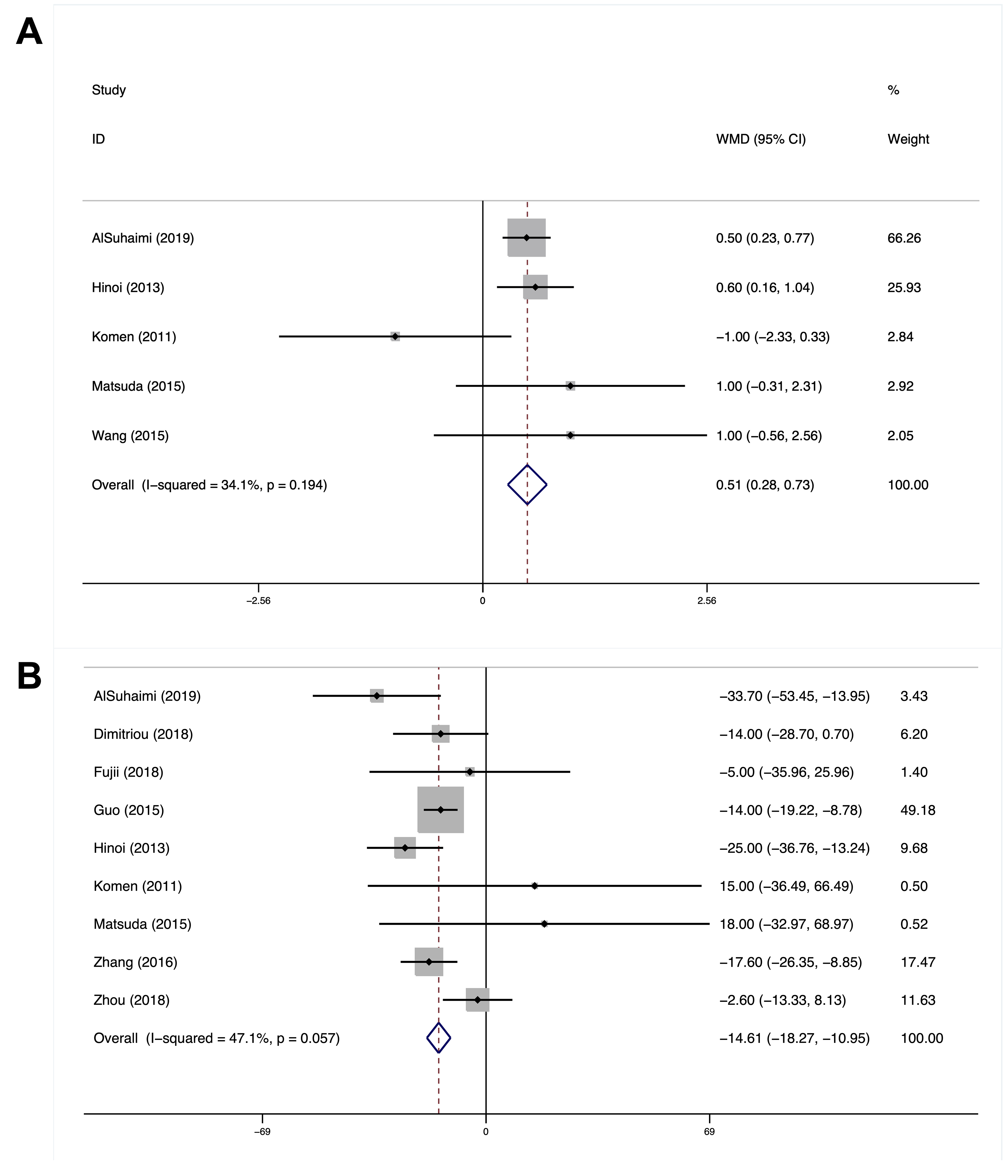
Lymph node dissection is a pivotal procedure in radical resection of CRC surgery [53]. The extent of lymph node involvement may be directly linked to the prognosis of CRC patients [54]. In LCA non-preservation surgery, the lymph nodes around the IMA should be removed as well, which could reportedly increase the number of lymph nodes harvested [55, 56]. In this case, regardless of whether the LCA should be preserved, the range of lymph node dissection would be theoretically the same and the number of the lymph nodes harvested would not differ, especially when new techniques to dissect the apical lymph node separately were introduced, as proved by our pooled results [56]. Regarding the number of metastatic lymph nodes harvested, our result showed that LCA non-preservation surgery can collect significantly more metastatic lymph nodes than LCA preservation surgery in both CRC and RC subgroups. This result might have been biased by non-RCTs on the assumption that high ligation tends to be performed in tumors with a higher N stage. However, detecting the difference in the N stage of cancers between the two groups was beyond the scope of this meta-analysis, which, we admit, is a limitation of this study.
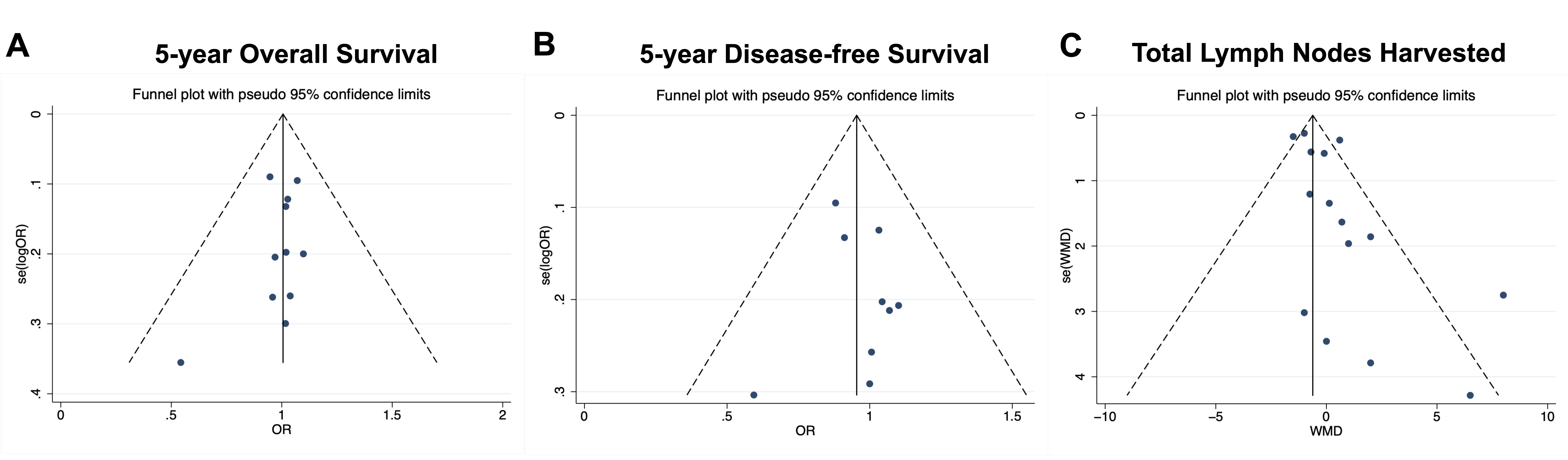
Moreover, the 5-year OS rate and 5-year DFS rate are critical outcomes for evaluating the prognosis of patients with malignancy tumors including CRC [57]. OS and DFS are associated with postoperative complications and the number of total and metastatic lymph nodes collected [39]. Non-preservation of the LCA can reportedly benefit the 5-year OS and DFS rates of CRC patients [12, 21]. In this meta-analysis, no difference in these two outcomes was found between LCA preservation and non-preservation in both the CRC and RC subgroups. The reason might be the better prognosis of CRC after radical surgery, and apical lymph node metastasis is rarely seen in most colorectal tumors. Therefore, it is essential to identify CRC patients with apical lymph node metastasis during preoperative assessment.
In this meta-analysis, the operation time in non-LCA preservation surgery is statistically shorter in the CRC group and RC subgroup. The exposure of the LCA in LCA preservation surgery is very challenging, and the dissection of the mesentery distal to the left colon in laparoscopic surgery is also time-consuming. In comparison, direct ligation of the LCA during surgery is easier, with downregulated difficulty of separating blood vessels, which enables operators to perform the surgery more efficiently and conveniently. A higher incidence of urinary dysfunction is reportedly associated with LCA non-preservation surgery in CRC [8], but no statistical difference was found in our study. The related nerve is located around the root of the IMA and could be preserved from damage if dissection and ligation were done carefully 1–2 cm away from the root of the aorta.
Nevertheless, this meta-analysis still has some limitations. First, both RCTs and non-RCTs were included in the analysis, making it difficult to formulate a more comprehensive and rigorous conclusion [6]. In the future, extensive and well-designed clinical trials, especially multicenter RCTs, are required to resolve this dilemma. Second, the subgroup of colon cancer could not be evaluated independently. Some conclusions regarding colon cancer were a combination of overall results and results of the RC subgroup, which makes it less reliable. Finally, few studies are still focusing on the apical lymph node dissection in LCA preservation surgery; thus, further research is needed to provide better evidence.
{kind=link}
{kind=link}
{kind=link}