This retrospective research developed an ANN model to predict PHER in HCC patients without macroscopic vascular invasion. This ANN model achieved satisfactory discriminatory and calibration capacities in both the derivation and validation cohorts, in addition to presenting greater prediction capacity than the conventional Cox model, existing recurrence models and commonly used staging systems. Moreover, the ANN model stratified patients into two risk groups, highlighting the significant differences between RFS in different risk groups.
The high incidence of PHER still represents a major challenge for clinicians [2–4]. Many previous researches had confirmed that early tumor recurrence was associated with intra-hepatic metastasis, while late tumor recurrence was closely related to multi-centric oncogenesis [6, 7]. Although adjuvant treatments were similar, patients with PHER have a significantly worse outcomes than patients with late recurrence [10, 11]. In order to prevent PHER and prolong the long-term survival of HCC patients, different researches have reported the effectiveness of different postoperative adjuvant treatments, including RFA, interferon, TACE and immunotherapy [16, 30, 31]. Ueno et al. [31] proposed that adjuvant TACE can reduce the PHER risk, but it cannot reduce the risk of late recurrence. Nevertheless, Jiang et al. [32] found that postoperative adjunctive TACE did not improve RFS and overall survival in HCC patients after curative liver resection. Ahmed et al.[33] suggested that TACE may worsen patients' quality of life. Furthermore, systematic reviews and meta-analyses also failed to provide strong evidence to support the application of these adjuvant treatments [34, 35]. These difficulties can be attributed to the heterogeneity of patient groups in several randomized and non-randomized controlled researches and to the resulting differences in adjuvant treatment outcomes. That is, if these researches focused only on the impact of adjuvant treatments on high-risk patients for postoperative tumor recurrence, the results would be different. Therefore, the identification of high-risk patients with PHER has an important clinical significance, which can become the focus of clinical researches on adjuvant therapies in the future. An accurate, reliable and specific prediction tool based on ready-made prognostic variables could accurately identify high-risk patients for PHER, thus constituting an effective method to address this clinical problem. This prediction model would be also closely related to monitoring of the recurrence of postoperative tumors. In theory, high-risk patients should adopt more aggressive and effective monitoring programs, such as the use of more accurate radiological researches to detect PHER. Thus, timely remedial measures can be taken. For example, some centers often perform preventive remedial transplants for high-risk patients after hepatic resection to prolong the long-term survival of HCC patients [36].
Many clinical and pathological prognostic factors have been shown to be the cause of tumor recurrence after curative hepatectomy. However, there are few studies on the establishment and detection of accurate and effective models for PHER prediction. To date, most of the proposed models have not focused specifically on PHER. These models included the recurrence clinical risk score of Lee et al. [37], Shanghai score of Sun et al. [38], recurrence score for hepatitis B virus-related HCC proposed by Qin et al. [39], a RFS nomogram for AFP negative patients performed by Gan et al. [40], early recurrence after surgery for liver tumour models built by Chan et al. [5], Hong Kong recurrent model developed by Ng et al. [8], recurrence after curative hepatectomy score constructed by Tokumitsu [41], and some radiomics-based prognostic prediction models [42–45], etc. Although these models are accurate, they were established using traditional linear models, such as Cox model and survival analysis. The correlation between different risk factors is multidimensional, complex and non-linear. Therefore, analyzes of the correlation between these factors present limitations when they are performed only by traditional linear methods. An ANN model is probably a more effective tool when multiple risk factors are involved in multidimensional and complex functions that interact with each other [12–16]. Here, we developed an ANN model based on the eight most important prognostic factors that performed better than Cox model and some existing recurrence models to predict PHER in HCC patients without macroscopic vascular invasion (Fig. 3 and Table 3).
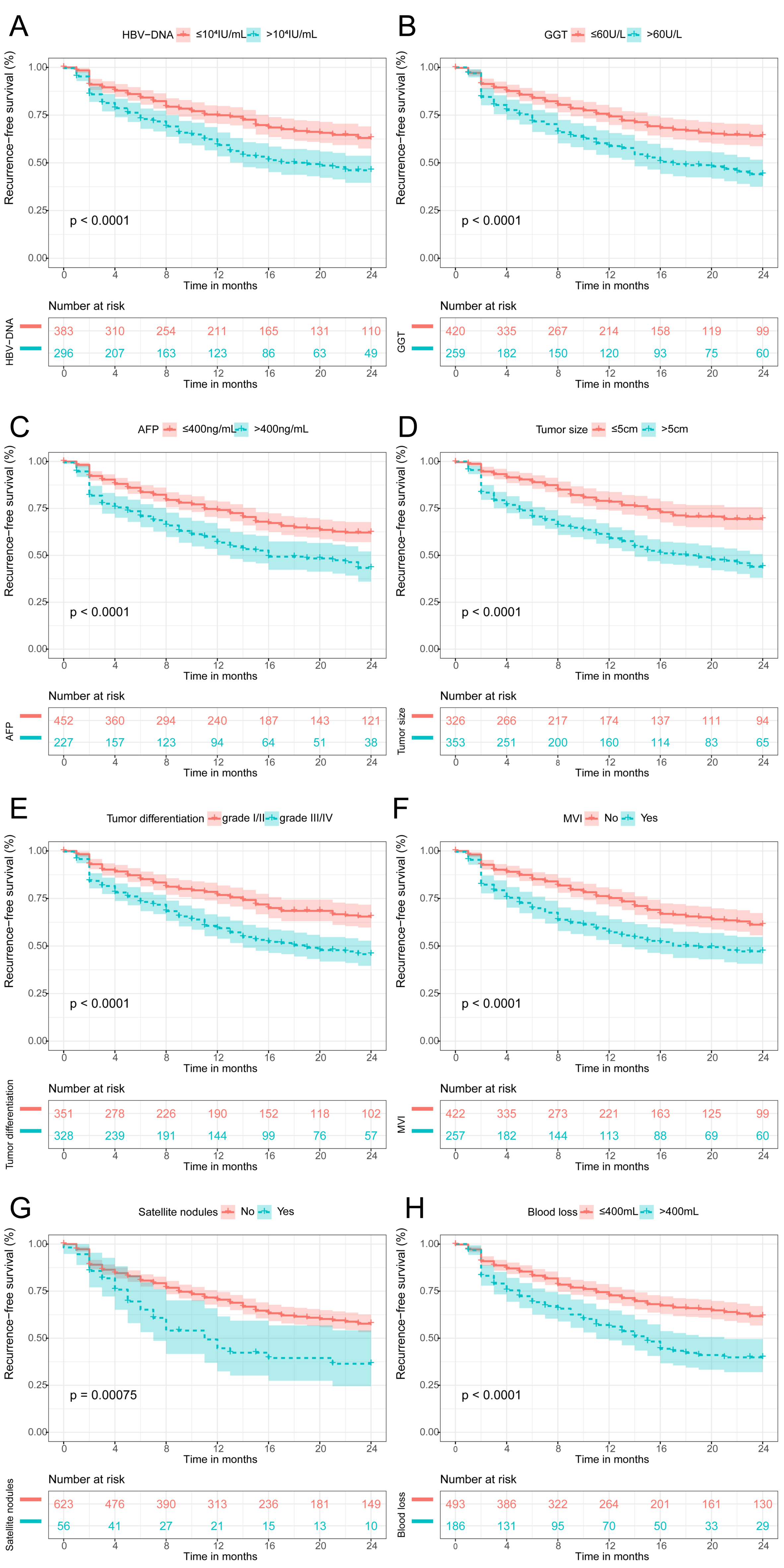
Our data revealed that HBV-DNA, GGT, AFP, tumor diameter, tumor differentiation, MVI, satellite nodules and blood loss were associated with PHER (Table 2). These factors are common and readily available in clinical practice. Previous data has shown that the higher the HBV-DNA load, the greater the risk of poor survival and tumor recurrence after hepatectomy [46–48]. High GGT levels may lead to liver dysfunction via inducing DNA instability, tumorigenesis and cancer progression. In addition, high GGT levels can predict the poor prognosis of HCC [49, 50] High AFP levels indicate that the tumor is highly aggressive as well as the probability of intra-hepatic metastasis being usually greater than in patients with low AFP levels[51]. Other studies have repeatedly reported that a larger tumour diameter is significantly associated with PHER [52] and that MVI, satellite nodules and tumor differentiation are related to worse PHER [53–55]. Finally, excessive blood loss often leads to systemic inflammatory reactions and reduces immunity, thereby increasing the risk of serious complications and tumor recurrence after surgery. All of these parameters are easily available in medical records, facilitating the routine use of ANN model in relation to other models that use complex radiological variables [42–45].
The ANN model obtanied in this work is more accurate in predicting PHER than commonly used staging systems (Fig. 3 and Table 3). This can be attributed to the fact that these systems and models contain very few parameters and try to balance the risk variables by summarizing them. Thus simplified models are obtained, which limits the accuracy of the PHER prediction in HCC patients. Moreover, these systems and models are also linearly additive forms based on prognostic variables, and the interactions between prognostic variables cannot be proven accurately. ANN models, on the other hand, contain a wide range of predictors and manage the interactions between all prognostic factors, helping to improve their predictive power.
Currently, there is no clear consensus or guidelines on the ideal adjuvant therapy after hepatectomy. In addition, the criteria for identifying high-risk patients for PHER are still unclear. Interestingly, the ANN model could be stored in the computer as a program. After the clinician enters these eight prognostic factors into the program, the computer will automatically and accurately calculate the risk of PHER. In this research, the ANN model cut-off value of 0.37 had a sensitivity of 72.0% and a specificity of 68.6% for assessing PHER risk. All patients were then divided into high-risk and low-risk groups. The risk stratification analysis showed significant differences in RFS curves between the different risk groups (Fig. 4, P < 0.001 for all). As expected, patients in the high-risk group had poor RFS, but screening these patients can be have a very positive impact on the use of adjuvant therapies strategies. For instance, in low-risk patients, appropriate adjuvant therapy should be accompanied by a reduction in side effects, especially in elderly patients. In contrast, high-risk patients may need to combine more adjuvant treatments to obtain optimal prognosis, particularly in younger patients. A recent meta-analysis showed that TACE + RFA can provide comparable therapeutic outcomes in HCC patients compared with hepatectomy and have the advantage of reducing morbidity[56]. This result is important for clinical decision making in high-risk patients, and it is worth considering whether a patient who is deemed to be high risk of PHER should not undergo a hepatectomy. Therefore, high-risk patients must be closely monitored and appropriate treatment options must be explored. Furthermore, the ANN model can allow stratifying the risk of PHER in patients more appropriately for the design of clinical trials. Despite the promising data presented here, it is relevant to recognize that the present study has some limitations. Most of patients evaluated here had HBV infection, therefore, further validation in other aetiological populations is necessary. In addition, this is retrospective study and was conducted with patients form a single medical center. Thus, prospective studies realized with patients form several medical centers are required to verify the results obtained.
{kind=link}
{kind=link}