Characteristics of the Study Population
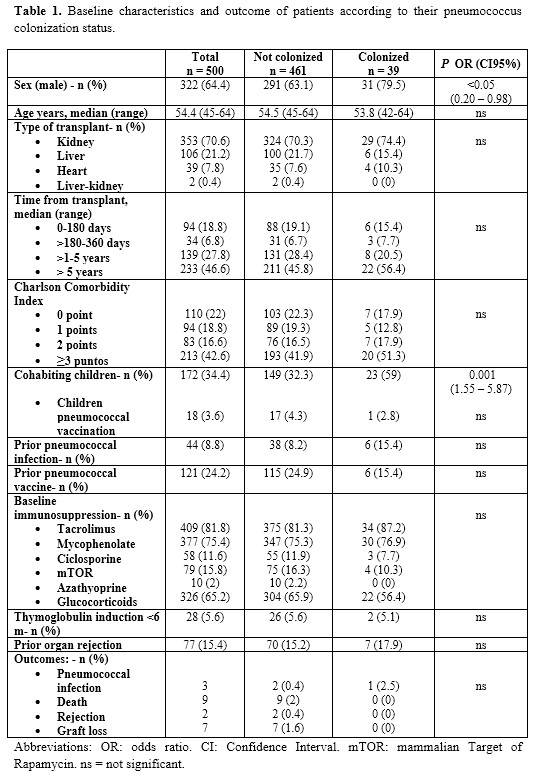
Five hundred SOT recipients were included in the study: 353 (70.6%) were kidney recipients, 106 (21.2%) liver recipients and 39 (7.9%) heart recipients. Most patients received tacrolimus, mycophenolate and steroids as immunosuppressant therapy. Twenty-four percent of patients reported having received pneumococcal vaccination. Clinical and demographic data are shown in Table 1. In winter 500 samples were collected, while in spring/summer 461 samples were. The difference in samples collection was due to 39 patients (7.8%) not attending to the spring/summer visit.
Pneumococcal Carriage and Infection
Twenty-six patients (5.6%) were colonized in winter and 15 (3.2%) in spring/summer (P=0.06). During the study period, three female patients (age range 53-71) were diagnosed with non-bacteremic pneumococcal pneumonia (Table 2); two of whom died.
The overall pneumococcal colonization rate in the 961 samples obtained was 4%. There were two patients with pneumococcal colonization in both studied periods. Colonized SOT recipients compared to non-colonized patients were more frequently men (79.5% vs. 63.1%, P<0.05) and cohabitated regularly with children (59% vs. 32.2%, P<0.001). In multivariable analysis these factors were also related to pneumococcal carriage: sex (men) OR 0.44 (CI95% 0.20–0.98) and cohabiting with children OR 2.90 (CI95% 1.5–5.77) (Table 3). There was no relationship between pneumococcal carriage and the immunosuppressant agents used, type of transplant or time since the transplant, pointing out that the immunosuppression was not related to the colonization status (Table 1).
Six colonized patients (15.4%) and 115 non-colonized patients (24.9%) had received pneumococcal vaccine prior to their inclusion (P<0.0.5). At the end of the study follow-up, 10 patients (2%) died; 7 (1.4%) lost the graft and 2 (0.4%) suffered an organ rejection. Colonized and non-colonized SOT recipients had similar outcomes regarding the incidence of pneumococcal disease, rejection, as well as graft and patients’ survival (Table 1).
Characteristics of Pneumococcal Isolates
During the winter period, 26 different serotypes were identified. The most prevalent serotypes were (in decreasing order): 35B (38.5%), 19A and 23A (11.5%), 6A/6B, 4, 6C/D, 9N/L and 23B (7.7% each) (Fig. 1). Overall, 52.7% of the winter isolates were included PCV23, while 47.2% were not included. Moreover, in 8 of the winter patients (30.8%) with pneumococcal isolates, no serotypes were identified by the molecular method used.
Sixteen isolates were resistant to azithromycin and erythromycin (36.36%), 15 isolates to clarithromycin (34.09%), 14 isolates to trimethoprim-sulfamethoxazole (31.82%), 2 isolates to oral penicillin (18.18%), and none to intravenous penicillin, amoxicillin, cefotaxime, ceftriaxone, levofloxacin and vancomycin (See Supplementary Table 1, Additional file 1).
In the spring/summer period, 15 different serotypes were identified, 35B (53.3%), 19A, 11A/D, and 38/25F (13.3%) (In decreasing order) being the most prevalent ones (Fig. 1). Moreover, 33.3% of the spring/summer isolates were included in PPV23, while 66.6% were not included. The serotype of a patient of the spring/summer period (6.7%) could not be identified with the molecular method used.
A reduction in the rate of antimicrobial resistance was observed in this period. Six isolates were resistant to trimethoprim-sulfamethoxazole (27.27%), 4 isolates to oral penicillin, azithromycin, erythromycin and clarithromycin (18.18%), and 2 isolates to amoxicillin (9.09%), and as in the winter period no isolate was resistant to intravenous penicillin, cefotaxime, ceftriaxone, levofloxacin and vancomycin (See Supplementary Table 2, Additional file 2).
The multiple-serotype carriage was similar in both study periods: 53.8% and 46.6%, respectively. Two patients were colonized during both periods with the capsular serotype 19A, and one of them was also colonized with the capsular 35B serotype in both periods.
Taking into account all the pneumococcal isolates collected in the study (n=57), the most frequent capsular serotypes were 35B (31.6%), 19A (8.77%) and 23A (7.02%). Twenty-six (45.6%) serotypes were included in any of the pneumococcal vaccines (PCV13 and PPV23), while 31 (54.4%) serotypes were not included.
On the basis of CLSI breakpoints, the percentages of resistant isolates were 30.3% for trimethoprim-sulfamethoxazole, azithromycin and erythromycin, 28.79% for clarithromycin, 9.09% and 3.03% for oral penicillin and amoxicillin, respectively. No resistance was observed in the cases of intravenous penicillin, cefotaxime, ceftriaxone, levofloxacin, and vancomycin (Table 4).
{kind=link}