Using a selective SERT PET radiotracer, we monitored a long-term SERT occupancy/recovery in vivo and evaluated the AMI neuroprotection after MDMA induction. Our results showed that acute and repeated administration of MDMA significantly induced SERT reduction levels in all regions at day 14 compared to the controls, which were supported by previous studies, revealing that the effect of MDMA on SERT binding was a robust finding in rodents [13, 20, 42, 43, 44]. Those reports indicate that the effect of MDMA on SERT binding is a robust finding in rodent.
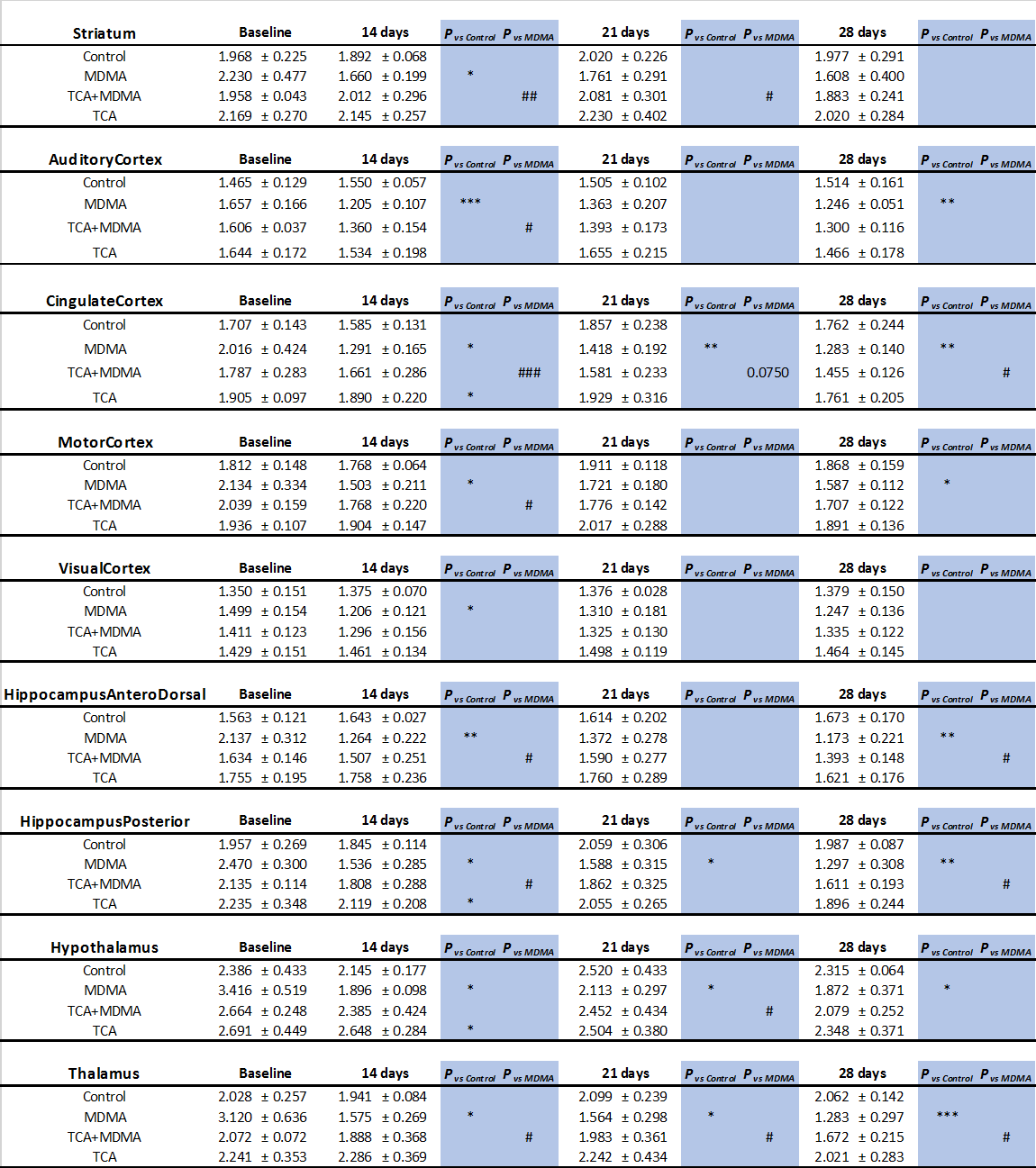
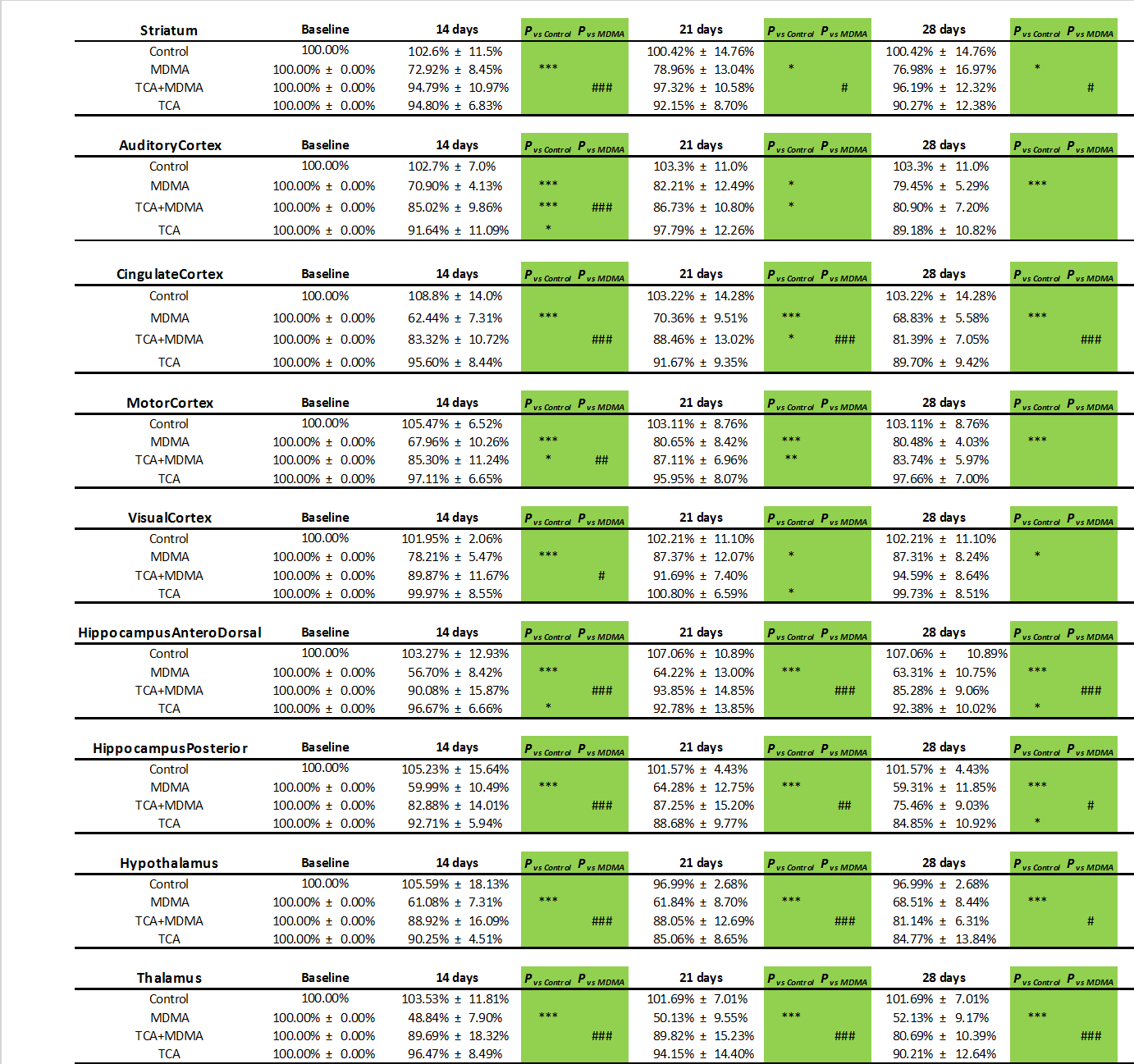
Regarding the long-term effects of MDMA exposure, we further investigated the effect of the duration of ecstasy abstinence on the SERT binding by examining the reversibility of the in vivo SERT binding during the period of abstinence from MDMA administration. We found that neurotoxicity induced by MDMA in rat brain was regional-specific, reflecting the varied SURs or progression of the self-recovery rate of SERT. In the study period (28 days), we found the regions, such as the thalamus, hypothalamus, hippocampus anterodorsal, and hippocampus anterodorsal (low or mid-self-recovery rate), had relatively slower self-recovery progression compared to cingulate cortex, motor cortex, auditory cortex, striatum, and visual cortex (high self-recovery rate) (Table 2 and Fig. 4). The results also indicated that the SERT self-recovery in rat brain after MDMA-induction was time-dependent and returned to 70.7% ± 3.96% of baseline values at day 28. The regions of low or mid-self-recovery rate were the most affected region by MDMA [4, 45].
In contrast, MacGregor et al., (2003) reported a clear loss of SERT binding sites in rats 3 months after administering the high-dose MDMA regime (4 × 5 mg/kg over 4 h in 2 consecutive days) [12], This agrees with numerous previous studies that show a SERT loss in the cingulate cortex, hippocampus, entorhinal cortex, medial hypothalamic area, and the medial and lateral thalamic nuclei of rats, following MDMA administration in a rodent model [46, 47]. Lew et al., (1996) reported that a progressive recovery of SERT binding was noted from 2 to 52 weeks following MDMA exposure [48]. Moreover, Li et al. (2010) reported < 50% SERT recovery rate using in vivo 4-[18F]-ADAMPET in the midbrain, thalamus, hypothalamus, caudate-putamen, hippocampus, and frontal cortex at day 31 after MDMA administration [20].
The difference in recovery time-course between the present study and previous reports described above could be (1) methodological issues that affected the accuracy of the quantitative measurement. For example, the reports published before 2000 used quantitative autoradiographic to analyze tissue slices or high-performance liquid chromatography (HPLC) for homogeneous tissue. However, the present study used PET imaging. (2) The analysis techniques, i.e. the accuracy of PET and MRI-based atlases registration or the correction of partial volume effect could underestimate the SERT binding in small volumes.
In a primate study, Scheffel et al. (1998) showed that SERT binding increased from 40 days to 9 months after MDMA administration in the pons, midbrain, and hypothalamus. However, it decreased in cortical regions [49]. Ma et al., (2016) reported that the SERT recovery rate was on average of ~ 66.6% and ~ 68.6% after MDMA administration in the striatum, thalamus, and midbrain at 24 and 54 months, respectively [13].
In human studies, some studies examined the reversibility of the SERT binding during abstinence from MDMA administration. Several reports demonstrated no difference in SERT binding between former ecstasy users and drug-naive controls after 1 year of abstinence [50, 51, 52].
Some preclinical or clinical studies confirmed a recovery in SERT binding after MDMA administration [40]. However, the question raised is the correlation between recovery of SERT binding and the function of SERT neurons. In the rat model, Andó et al. reported that 6 months after administering high-dose (15 or 30mg/kg, i.p), MDMA-induced damage of serotonergic axons showed recovery in most brain areas. However, SSRIs reduce serotonergic functions. Anxiety and aggression remain altered [53]. Li et al., (2010) suggested that when the SERT recovery rate reached ~ 35.2% compared to the controls, the density of serotonergic fibers and cell bodies decreased at day 31 after MDMA treatment (10 mg/kg, i.p) [20].
In the human study, several studies reported that after one year of abstinence, ex-MDMA users showed deficits in the Rey Auditory Verbal Learning Test similar to current MDMA users although SERT binding was similar to control level [50]. A review of empirical research (2013) supported those cognitive impairments following MDMA administration, which could result in a long-term cognitive effect, such as retrospective memory, prospective memory, higher cognition, problem-solving, and social intelligence. It can also result to sleep architecture, sleep apnoea, complex vision, pain, neurohormones, and psychiatric status [54].
Golding et al., (2007) reported that light ecstasy users showed a small significant cognitive impairment. However, no such impairment was detected among ex-users absent from the drug for at least 6 months [55]. Thus, neuroimaging studies show reduced serotonin transporter levels across the cerebral cortex, associated with neurocognitive impairments. SERT recovery positively correlates with the duration of MDMA abstinence. However, it is unclear whether the cause is associated with the SERT neurons recovery or other causes. Future longitudinal studies are recommended to investigate the serotonin level in blood or cerebrospinal fluid [45] or behavior tests.
The present results demonstrated that co-administration of MDMA with AMI rapidly blocked MDMA-induced serotonin release and MDMA neurotoxicity, restored globally, and largely accelerated SERT levels at day 14. After day 14, the progression of SERT recovery rate increased slowly at a rate of approximately 3% per 7 days and reached ~ 70% of baseline at day 28. Among all regions, those regions with low or mid-self-recovery rates had weaker responses to AMI when compared to regions with high recovery rates.
Li et al., (2010) reported that co-administration of MDMA with SSRI, fluoxetine, restored SERT binding rate to ~ 79.6 % of the control level at day 31 post-MDMA [20]. Compared to fluoxetine in the current results, AMI showed a 84.38% ± 2.05% of recovery rate at day 28. AMI had a higher neuroprotective effect because of its antiapoptotic effect that prevented PC12 cell death caused by hydrogen peroxide [56]. Another reason could be that MDMA can cause hyponatremia that induces seizures [57], resulting in an anoxic brain. However, AMI can protect primary cultured hippocampal neurons and in vivo hippocampal neurons from oxygen-glucose deprivation-induced apoptosis [34]. Moreover, AMI showed significant improvement in long- and short-term memory and increased neurogenesis and neurosynaptic marker proteins in an AD mouse model [32]. However, MDMA can influence a long impact on cognitive impairments.
Cytochrome P450 2D6 is the main enzyme involved in MDMA metabolism [58], and the AMI is a potent inhibitor of the Cytochrome P450 2D6 enzyme [59], which may inhibit MDMA metabolism and increase the MDMA toxicity.
In contrast to the expensive, risk-overt, and time-consuming nature of de novo drug development, a more effective approach is to apply the well-tolerated, therapeutics in new pharmacogenomic settings. Seeking effective treatments in Food and Drug Administration-approved drugs has become a promising drug discovery route for neuroprotection by MDMA.
Our findings in immunochemical staining confirmed the PET study, revealing that at day 28 post-MDMA, the density of serotonergic fibers and cell bodies decreased in the MDMA group. On the contrary, co-administration of MDMA with AMI showed improvement in structural damage of serotonin neurons (Fig. 5–6). After being measured by RT-PCR, our results supported a decrease in SERT gene expression in the striatum, parietal cortex, and hippocampus after MDMA treatment [60]. The results were consistent with several studies that reported dramatic decreases in SERT binding following various MDMA dosing regimens and post-administration [61]. This previous study also showed the effect of MDMA on SERT depletion region-specific. For example, areas such as the striatum, raphe nuclei seem to affect stronger than other areas such as the hypothalamus. In the long term, the evidence suggests that SERT gene expression is negatively regulated by MDMA exposure [62], leading to reductions in SERT binding and immunoreactive fiber density in the absence of physical damage.

{kind=link}
{kind=link}