The key finding of this study is that elevated preoperative procalcitonin, along with other preoperative factors such as age, depression, and compromised daily functioning, accompanied by prolonged CBP time, are the most critical factors in the development of postoperative delirium after cardiac surgery. To our knowledge, this is the first study showing the usefulness of procalcitonin as a predictor of the development of postoperative delirium in patients undergoing cardiac surgery.
In the present study, it was observed that patients who experienced postoperative delirium had higher procalcitonin levels both before surgery and on the following days, compared to patients without delirium. PCT is a peptide precursor of calcitonin and a biomarker of inflammation. In ICU patients, PCT has been used to identify bacterial infections and monitor antibiotic therapy as part of standard care for septic patients. Procalcitonin levels may arise in the course of the inflammatory reaction in response to surgical trauma without infection, and a transient increase in the PCT level has been observed even during uncomplicated heart surgery [24]. In cardiac surgery, the systemic inflammatory response can be activated by many factors such as surgical trauma, CBP circuit, endotoxemia, and ischemia-reperfusion injury. Various inflammatory mediators, including PCT, are released and lead to systemic effects such as vasodilatation and disturbances in the microcirculation [10]. Long CBP is a powerful inductor of a systemic inflammatory reaction, and brain function may also be affected. Consistent with the neuroinflammatory hypothesis of postoperative delirium, inflammatory mediators released when the systemic inflammatory response has been activated cross the blood-brain barrier, activating microglial cells to produce inflammatory mediators. Consequently, damage to brain tissue, dysfunction of neuron activity, disturbances in the neurotransmitter system, impaired synaptic conduction, and leaking of intercellular connections of blood-brain barrier cells were detected [9] [25].
Here, we assessed PCT because daily PCT measurements are readily available as part of routine in-hospital monitoring, and the predictive value of PCT for diagnosing complications after cardiac surgery had been previously confirmed. Clementi et al. presented results that the PCT measurement performed 48 hours after the cardiac operation was a good predictor of postoperative renal and respiratory complications [14]. In another study, Klingele et al. showed that a single PCT measurement taken the day after surgery was a predictor of delayed complications such as prolonged hospitalization, ICU readmission, and hospital death [26].
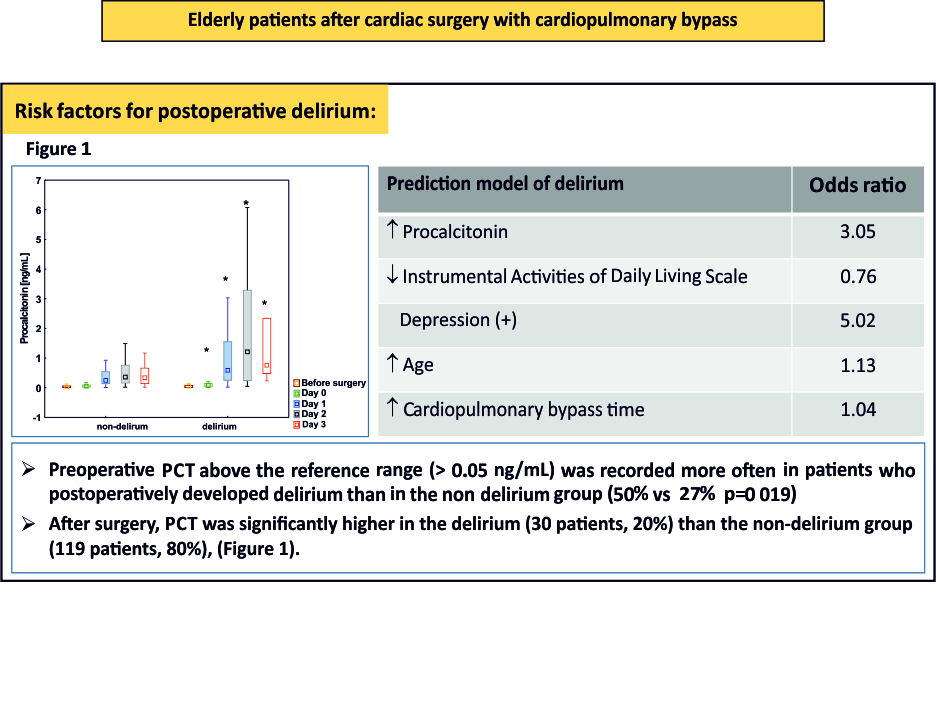
The importance of procalcitonin as a predictor of delirium has not yet been established. Earlier, McGrane et al. demonstrated that in a population of non-cardiac ICU patients, high PCT values recorded on ICU admission predicted prolonged periods of acute brain dysfunction, linking inflammation as an essential mechanism in the pathophysiology of delirium [27]. In a later prospective study by Nemeth et al., the relationship between changes in the procalcitonin concentration measured on the first day after surgery and the occurrence of postoperative cognitive dysfunction was assessed in a population of elderly patients undergoing on-pump cardiac surgery, and no relationship was found between inflammatory response and cognitive dysfunction [28]. In this study, according to the multivariate logistic regression analysis, a PCT concentration above normal before surgery significantly increased the risk of postoperative delirium with an odds ratio of 3.05 (p = 0.048) in a population of patients undergoing cardiac surgery. After the operation, the median level of PCT was elevated with a peak value on the second day. This observation was expected and could be explained by the activation of a systemic inflammatory response during surgery. However, it should be emphasized that in patients with postoperative delirium, PCT was significantly higher than in patients without delirium during the entire follow-up. These observations confirm the utility of PCT measurements in predicting delirium. A PCT test is readily available (hospital laboratory, point of care testing), fast, and relatively cheap; therefore, a measurement before and after operation may be an additional indicator useful for the early identification of patients at risk for postoperative delirium.
The causes of delirium are multifactorial. According to multivariate logistic regression analysis, the best model for predicting delirium development after cardiac surgery included the preoperative PCT concentration, IADL score, the presence of depression, age, and the duration of CPB. The elderly are particularly sensitive to the development of postoperative delirium; in addition, delirium duration is longer in elderly patients than in younger patients subjected to cardiac surgery. Previously, Cereghetti et al. found that each year of life significantly increased postoperative delirium risk with an OR of 1.06 [29]. These results coincide with our research; according to the multivariate logistic regression analysis, the patient’s age was a significant factor of the model that predicted postoperative delirium with an odds ratio of 1.13.
Depression is frequent in older people and seems to be another critical risk factor of postoperative delirium. We reported here that the presence of preoperative depression was associated with a 5-fold increased risk of postoperative delirium. A study by Eshmawe et al. confirmed that a higher preoperative depression score was associated with an increased risk of postoperative delirium [30]. In another study, Oldham et al. demonstrated a relationship between the occurrence of preoperative depression and the development and severity of delirium after CABG. The authors used three different scales to diagnose depression, and only one scale (Patient Health Questionnaire 9) was predictive of delirium, while the results of two other scores (GDS-15 and HDRS) were shown to have little or no association with postoperative delirium [31]. Different scales have been used to measure depression, and it remains unclear which measure of depression may be most predictive of outcome.
Advanced age is one of the most important risk factors for functional deterioration assessed by the IADL score. It was estimated that 40% of men and more than 50% of women were limited in at least one IADL activity [32]. A decline in physical activity such as doing housework, travel, and shopping were more age-dependent than cognitive activities such as using a telephone, managing finances, or taking one’s medication [33]. In our research, patients who developed postoperative delirium had significantly compromised physical activities assessed with the IADL score. Moreover, in the multivariate logistic regression analysis, a lower IADL score estimated before surgery was a significant risk factor for postoperative delirium. These results confirm the importance of examining depression or the deterioration of physical and cognitive activity before an operation in an elderly patient. As part of a comprehensive geriatric assessment, tools such as the IADL and GDS-15 should be a routine part of managing an elderly population to help identify cases of increased risk of postoperative delirium.
Comorbidities are known risk factors for the development of postoperative delirium [34]. In our study, a majority of patients were diagnosed with arterial hypertension; diabetes and chronic renal insufficiency were common. Except for anaemia, there was no difference in the distribution of comorbidities between groups. Anaemia was diagnosed in 43% of patients in the group who developed postoperative delirium, and only 19% in the group without delirium. Previous studies have shown that preoperative anaemia was considered a risk factor for the outcome in non-cardiac surgery; it was associated with a more extended hospital stay, a higher risk of perioperative complications, and higher mortality [35]. In a recent study of 800 patients undergoing elective non-cardiac surgery, anaemia was associated with postoperative delirium and longer hospitalization [36]. The impact of preoperative anaemia on postoperative delirium in the cardiosurgical population is not yet well understood, and the results published so far have often been contradictory. In a systematic review based on 34 studies, several studies identified anaemia as an important risk factor for delirium following on-pump cardiac surgery, while others did not find an association [37]. In a recently published study by Smulter et al, the preoperative haemoglobin level was not associated with postoperative delirium [38]. In our study, preoperative anaemia was more than twice as common in the group with postoperative delirium than in patients without delirium (43 vs 19%, p = 0.006); however, in a multivariate logistic regression analysis, the presence of preoperative anaemia was not included in the prediction model. It seems that this issue requires further evaluation in larger populations.
In the present study, more patients who postoperatively developed delirium required a complex procedure. This resulted in a significant prolongation of CBP time. Along with long aortic cross-clamping, prolonged CBP time has been one of the most important factors of postoperative delirium [6]. This observation was also confirmed in our study in the multivariate logistic regression analysis. The duration of CPB was a significant factor in the model predicting postoperative delirium with an odds ratio of 1.04. This observation leads to the conclusion that qualifying elderly patients for long and complex procedures require careful consideration and balancing the risks and potential benefits.
Our study has several limitations. First, we didn’t assess the long term consequences of delirium, postoperative cognitive decline, or a reduced quality of life after the operation. Second, our model was based on patients in one centre. Multi-centred research on the assessment of procalcitonin and other inflammatory markers is worth considering.
{kind=link}
{kind=link}
{kind=link}