SRH is a relatively rare clinical entity that involves bleeding in the retroperitoneal space without any triggers. SRH usually occurs in the population taking anticoagulants [1]. However, our patient was not taking any anticoagulant or antiplatelet medications. Bleeding can occur in any retroperitoneal vessels and organs [2]. Although the pathogenesis of SRH is unclear, it may be caused by arteriosclerosis of microvessels [2], vascular lesions like segmental arterial mediolysis [3], or unrecognized minor [2] trauma. The cause of bleeding is often unclear.
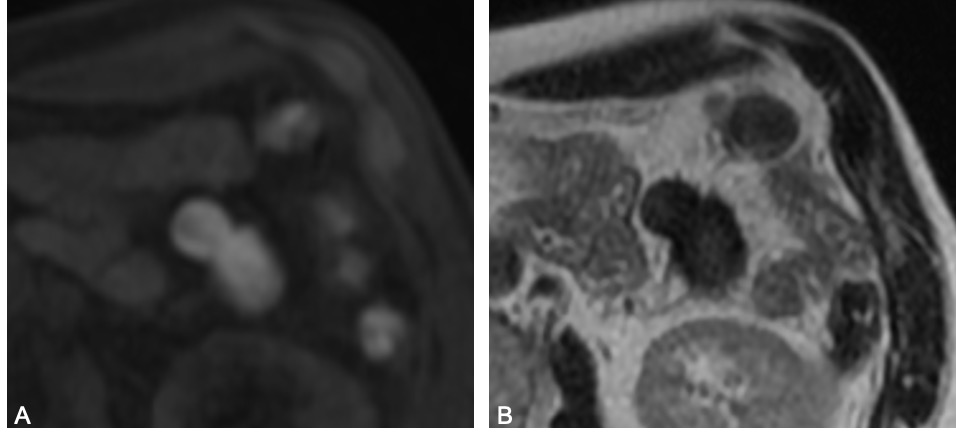
CT is a rapid and readily available test to identify retroperitoneal hematoma [4]. Extravasation is an independent predictor for TAE or surgical intervention [5]. MRI is helpful in establishing an accurate diagnosis owing to its efficient detection of retroperitoneal structures, including fat, organs, tumors, and hematoma [6]. Although MRI is not always necessary for diagnosis in the acute phase, it may be useful for differential diagnoses. Angiography is effective for detecting the hemorrhagic site and can enable the embolization of the affected arteries to stop the bleeding [7]. In the present case, contrast-enhanced CT revealed a low-density area in the central and left retroperitoneal space; however, neither extravasation nor causative aneurysm was observed. Enhanced MRI revealed heterogenous low T1 and high T2 signals indicating hematoma. Hence, the patient was diagnosed with SRH.
We present the diagnostic and management algorithm of SRH based on a literature review (Figure 3). If the bleeding occurs because of aortic aneurysm rupture, urgent endovascular aneurysm repair (EVAR) or open surgical repair is required [8]. Retroperitoneal hematoma can be treated conservatively when there is no persistent bleeding and the circulation is maintained, whereas endovascular or surgical treatment is required when the circulation is unstable [2]. When the circulation is stable with continuous transfusion or vasopressor infusion, ongoing bleeding is suspected [9], and dynamic enhanced CT should be performed again.
Most patients with retroperitoneal hematoma take anticoagulant and/or antiplatelet medications. Discontinuation of these antithrombotic agents and the reversal agents, such as vitamin K, idarucizumab, and prothrombin complex concentrate, are recommended [10]. In the presence of congenital or acquired hemophilia, active prothrombin complex concentrate and recombinant factor VIIa should be administered [11]. The European guideline on the management of major bleeding and coagulopathy following trauma states that in cases of hemorrhagic shock, fluid resuscitation should be started and vasopressors, including norepinephrine, can be administered to achieve systolic blood pressure of 80–90 mmHg [10]. Transfusion is required to maintain Hb level of 7–9g/dL and platelet count above 50 × 109/L [10]. The guideline also recommends treatment with fibrinogen concentrate or cryoprecipitate when Clauss fibrinogen level are ≤1.5g/L [10]. Fresh frozen plasma (FFP) administration is suggested if prothrombin time and/or activated partial thromboplastin time are >1.5 times the normal values [10]. In this case, the patient was in hemorrhagic shock, and the bleeding seemed to be persistent; however, his blood pressure could be maintained by fluid resuscitation, vasopressor infusion, and blood transfusion. Enhanced CT did not show extravasation and the bleeding site. Angiography was not performed because the possibility of active bleeding was less likely and embolization of the causative arteries was not necessary. Conservative management with close monitoring in the ICU was chosen so that urgent TAE or laparotomy could be performed in case of prolonged and worsening shock state resulting from rebleeding. The retroperitoneal cavity is a relatively narrow space, and the tamponade effect of the hematoma reportedly stops bleeding [2]. Sunga et al. reported that the overall mortality of SRH within 30 days was as high as 10.1% [1]. Because of the high mortality rate, SRH cases need to be monitored carefully.
Tani et al. reported that in a retrospective study of 20 consecutive cases of SRH, TAE could achieve hemostasis in 17 out of 19 patients [7]. In four of these patients, the causative arteries could not be identified, and the arteries around the hematoma were embolized empirically [7]. Even if the origin of bleeding is not detected, empirical embolization might stop life-threatening bleeding. In this case, angiography was not performed because the patient was hemodynamically stable following fluid resuscitation and vasopressor infusion and had significant renal dysfunction due to dehydration.
Surgical treatment is performed to stop the bleeding and remove the hematoma [2]. Emergency laparotomy is indicated in cases of abdominal compartment syndrome and compression of the lumbar plexus or femoral nerve [12]. In a report of cases in which surgery was performed prior to TAE, the bleeding site was not intraoperatively identified in all of the four patients [13]. If the bleeding site cannot be identified, intra-abdominal packing can stop the retroperitoneal bleeding, and reoperation can be planned after 48 hours [10] for re-examining whether hemostasis is achieved [2]. In the hemodynamically unstable emergency cases, TAE should be performed in a hybrid operating room, and if the bleeding cannot be stopped by TAE, emergency laparotomy is needed.
We report a rare case of SRH with unstable hemodynamic status that was successfully managed via conservative treatment with close monitoring. As the mortality rate of SRH is high, SRH management requires systematic and close monitoring based on our suggested clear evaluation criteria and management algorithm.
{kind=link}