TNT-mediated inter-cellular connections. TNTs are tubular structures of nanometer-to-micrometer diameters that connect the cytoplasm of adjacent or distant cells, thus providing an intracytoplasmic passage to exchange and/or transport biomolecules as small as ions, lipids, nucleic acids, microRNA, cytoplasmic proteins, or as big as whole organelles, such as endosomes, lysosomes, mitochondria and portions of the endoplasmic reticulum or Golgi apparatus. They can be very long, notably over submillimeter distances (spanning several cell diameters)29–36. TNTs are reported to be transient structures and can form or disintegrate in a matter of a minutes29. They are documented to promote the spread of various pathogens, including viruses37,38, prions39, fungi40 and mycoplasma41.
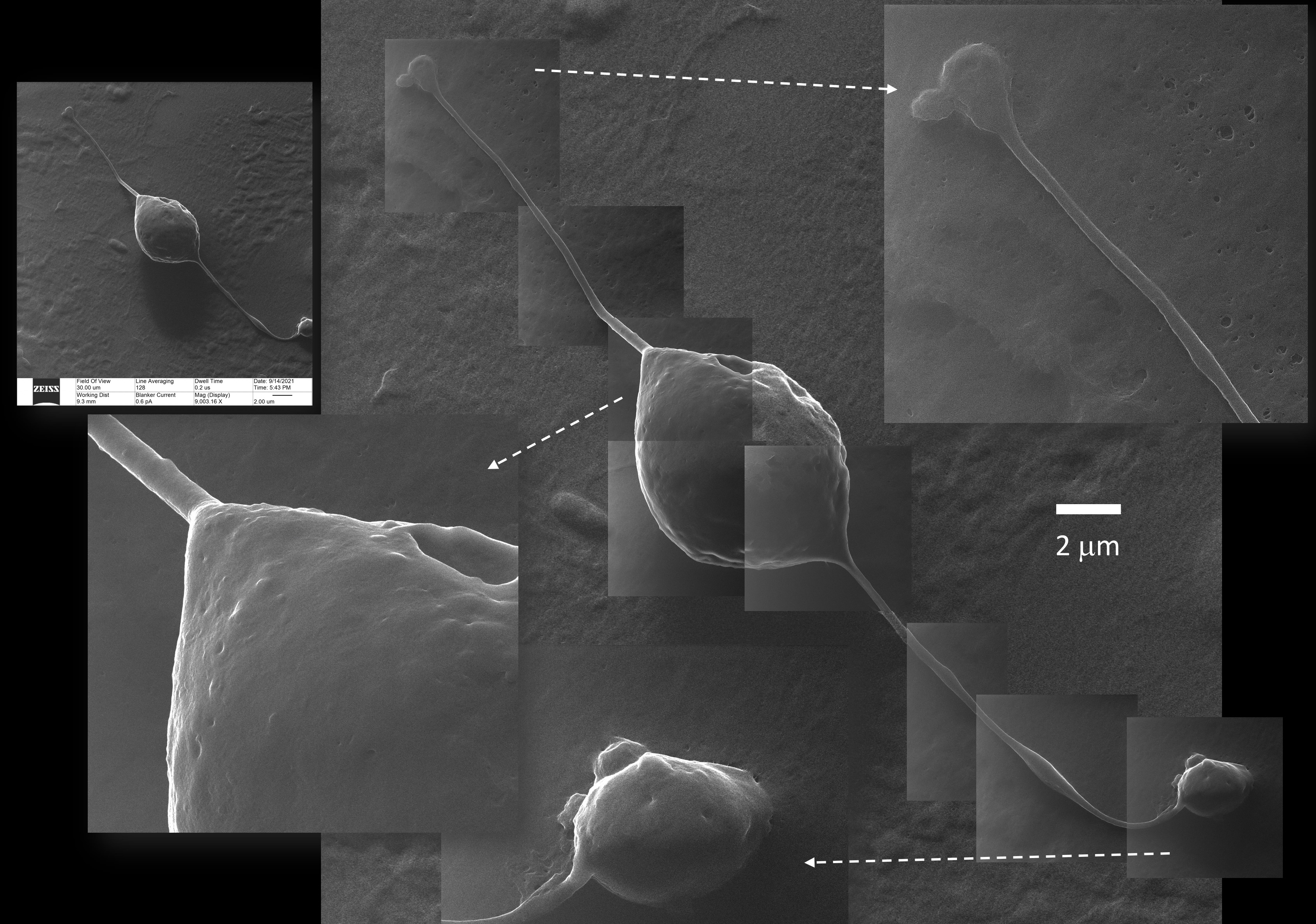
TNT were initially hypothesized as a subset of filopodia, but accumulating evidence suggests that TNT are categorically different from filopodia, both in length (longer than filopodia), diameter (as thin as filopodia but as large as axons), composition and function. Unlike TNT, filopodia are not capable of mediating vesicular transport. Filopodia are made of F-actin, while TNT, despite being composed of F-actin in their vast majority, can incorporate microtubules too, or be mainly composed of microtubules42. Some authors have named long-filopodial bridges containing F-actin as “cytonemes” and differentiated them from TNT43–45. We recognize that TNT is now the most accepted term in the literature, even if there are structural variations among them that may justify a further sub-classification. With their growth cone, length, potential microtubule skeleton, and intraluminal transport, TNT resemble the neuronal axons46. TNTs may form gap-like junctions between two connected cells over a short distance and extend when the two connected cells migrate apart. We documented this mechanical stretch, the capability of TNT to withstand it, and the presence of bulging(s) mid-way. While it is possible that this bulging represents a fusion of two growth cones originating from different cells, or some other phenomenon associated with intraluminal cargo transport, it is also likely that the bulging is just a physical response to the stretching and thinning of the nanotube47. TNT may keep its structure when overlapping cells are present in between the two distant cells that they connect. However, we documented the occurrence of possible membrane fusion of overlapping TNT with cells in between, thus suggesting the possibility that the cytoplasm of multiple cells may be connected through a single TNT. Like in axonal transport, TNT diameter enlarges when a bulky content is transported inside. The spherical morphology of some of these contents has been clearly captured by HeIM, which suggests that the transport of vesicles or viral particles is possible through TNTs.
The role of TNTs in SARS-COV-2 infection has been discussed in two recent papers32,33. TNT-mediated intracellular spread can protect the viruses from the circulating immune surveillance and possible viral-neutralization activity present in the extracellular matrix. Intercellular viral spread via TNT avoids virus-cell interactions that may initiate host defense signaling and mount antiviral responses. Many viruses, such as the influenza virus, human immunodeficiency virus (HIV), and herpes simplex virus (HSV), can evade host immunity and avoid pharmaceutical targeting by using TNT to transmit their genomes to naïve/new cells. Our observations using HeIM images make it reasonable to add SARS-CoV-2 to the list of viruses that can transmit and cause infection between host cells through TNT. Consistent with this notion, we did not observe any TNT formation in the uninfected Vero E6 cells.
Cell fusion. Cell-cell fusion (a.k.a. Syncytia) can be induced by certain types of viral infections, such as HIV, respiratory syncytial virus, and HSV48. Syncytia formation has been reported in the literature associated with SARS-COV-2 infection49–51, most notably in histopathologic lung sections from patients who died from COVID-1951. Another relevant finding is that Vero E6 cells, upon expressing the SARS-CoV-2 spike protein, could form syncytia as long as the ACE2 is present, but they cannot when transfected with SARS- CoV spike protein50, implying that cell fusion capability may be specific to SARS-CoV-2. It is reasonable to think that virus-induced cell fusion can facilitate the transfer of the viral genome to the neighboring cells49 by sharing cytoplasm between the cells. We observed significant Syncytia events only in the SARS-CoV-2 infected Vero E6 cells and not in the uninfected cells.
Extracellular vesicles. Cell-cell communication can be mediated by factors released in the intercellular space, such as hormones, cytokines, and other inflammatory mediators. The general term extracellular vesicles (EV) refers to any membrane vesicle released into the extracellular space. An accepted classification defines vesicles generated inside the cell and released into the extracellular space as “exosomes,” (diameter range from 30 to 150 nm). In contrast, vesicles pinched off from the plasma membrane are called “microvesicles” (diameter range from 150 to 1000 nm)52,53. Some Authors consider apoptotic bodies (bulk protrusions from dying cells that may end up in extracellular vesicles of 800nm diameter or larger) as part of the EV family. For a long time, EV were considered as “cellular dust” and did not attract much attention from researchers53. However, EV have recently been found to play key roles in cell-cell communication, allowing cells to exchange proteins, lipids and genetic material27,54.
Viruses might use EV to infect naïve/new cells55. The physical and chemical characteristics of many EV, as well as their biogenesis pathways, resemble those of retroviruses. EV generated by virus-infected cells can incorporate viral proteins and fragments of viral RNA, which is similar to the defective (noninfectious) retroviruses. EV are known to facilitate HIV-1 infection and dissemination; HIV-1 has been reported as “entrapped” in exosome aggregates56. “Trojan” exosomes might provide retroviruses the ability to take advantage of the cell-encoded intercellular vesicle traffic56–58. HIV-1 exploits the surface properties of the exosomes to facilitate rapid infection of progeny virus, and in so doing, camouflages the virus from immune surveillance. Surrounding itself with exosomes, HIV-1 can accelerate its infection and dissemination56. It has been hypothesized that SARS-CoV-2 infected cells can release EV with viral antigens or cargo. EV acting as a “Trojan horse” could explain the re-appearance of the viral RNA in patients recovered from COVID-19 28,59. EV are involved in SARS-CoV-2 infection60–62 and could be used as biomarkers of disease severity63. SARS-CoV-2 RNA has been identified in the exosomal cargo of samples from patients with COVID-19, but not in healthy subjects, suggesting that the virus might use the endocytosis route to spread infection64.
Extracellular vesicles can convey pathogen molecules that serve as antigens or agonists of innate immune receptors to induce host defense and immunity or serve as regulators of host defense and mediators of immune evasion54,56. We speculate that the mechanism of camouflaging the virus from immune surveillance might rather trigger an autoimmune response from the host in those instances where the close association of viral and host antigens promotes their crossed-recognition.
The intra-cytoplasmic route of SARS-COV-2 transmission. The nanometer resolution, lack of coating and practical imaging of samples provided by scanning HeIM suggest that SARS-CoV-2 infected Vero E6 cells can establish connections by TNT. HeIM also confirmed that they could form syncytia and exchange EV. These three features co-exist together in space and time. In all three processes, there is an exchange of cytoplasmic content between host cells. This may likely be an alternative route of transmission and infection, clearly distinct from the well-known, conventional extra-cytoplasmic ACE2 (or other receptor-mediated) docking mechanism. Even if the close phylogenetic relationship between SARS-CoV and SARS-CoV-2 makes it reasonable to translate much of our knowledge of SARS-CoV to SARS-CoV-2, we should focus on the differences between SARS-CoV and SARS-CoV-2 to explain divergent clinical patterns of disease caused by these two viruses. We already cited the fusogenic potential specific to the SARS-CoV-2 spike protein, but not the SARS-CoV spike protein50. Notably, SARS-CoV-2 has a lower density of spikes and can produce a high number of defective copies (with little or no spikes) released outside the infected cell65,66. These observations seem like strong, even if indirect, evidence that an alternative route of viral propagation must be in place for SARS-CoV-2.
The intra-cytoplasmic route can hide the virus from the host immune surveillance and potential anti viral response, based on the detection of the extracellular virions. In the intra-cytoplasmic route, naïve cells could be infected by viral mRNA, transmitted free, or in the form of cargo in micro-vesicles. Defective virions, presenting little or no spikes, which would be defective to infect other cells via the extra-cytoplasmic route, might become infective when transmitted via the intra-cytoplasmic route. Host defenses based on a humoral or cellular immune response are mostly ineffective against this intra-cytoplasmic spreading of SARS-CoV-2. More than two decades of failure to realize a protective vaccine for HIV highlights the need for a better understanding of the viral immune evasion mechanisms56, and we wonder if a similar case is mounting for SARS-CoV-2.
Clinical relevance. The vast majority of diseases, including COVID-19, are complex in their disease presentation and have multiple stages, and each stage may have a specific/targeted and generic/multiple targets therapeutic approach (many forms of cancer fit in this description). Specific drugs that interfere with the intra-cytoplasmic route of viral transmission described in this report can be promising therapeutic candidates to treat COVID19. Analyzing the spectrum of possible therapeutic molecules that impair the intracytoplasmic route of viral transmission is beyond the scope of this paper. However, we report that some suitable drugs have been tested already. In targeting TNT, the proven clinical efficacy in treating COVID19 of Colchicine, a microtubule inhibitor that might interfere with TNT formation67,68, can be suggestive evidence of the role of TNT in COVID19 pathogenesis. Drugs that suppress cell fusion have been tested in vitro51; among them, niclosamide, an oral anti-helminthic agent, was effective in cell protection against virus-induced cell death49,51. Drugs that interfere with EV machinery at large have been tested even before the COVID-19 pandemic. Chloroquine is well-known for elevating endosomal pH and has been shown to be effective against SARS-CoV infection in vitro69 and in COVID-19 cases70. In their interference with the cytoplasmic route, these drugs likely need to be administered during the early stages of SARS-CoV-2 infection and should be considered to have a limited or no preventive capability.
Limitations in our study include the absence of wider use of specific markers to track the viral transmission and usage of primary human cells to confirm our findings. However, observations reported here are actually stimuli for planning new studies not only by us but also by the larger scientific community. Having highlighted the presence of a potential intracytoplasmic route for SARS-COV-2 transmission and infection can provide a pathophysiological explanation for how therapies already in use may work and promote efforts towards the identification of new therapeutic agents.
{kind=link}