Subjects
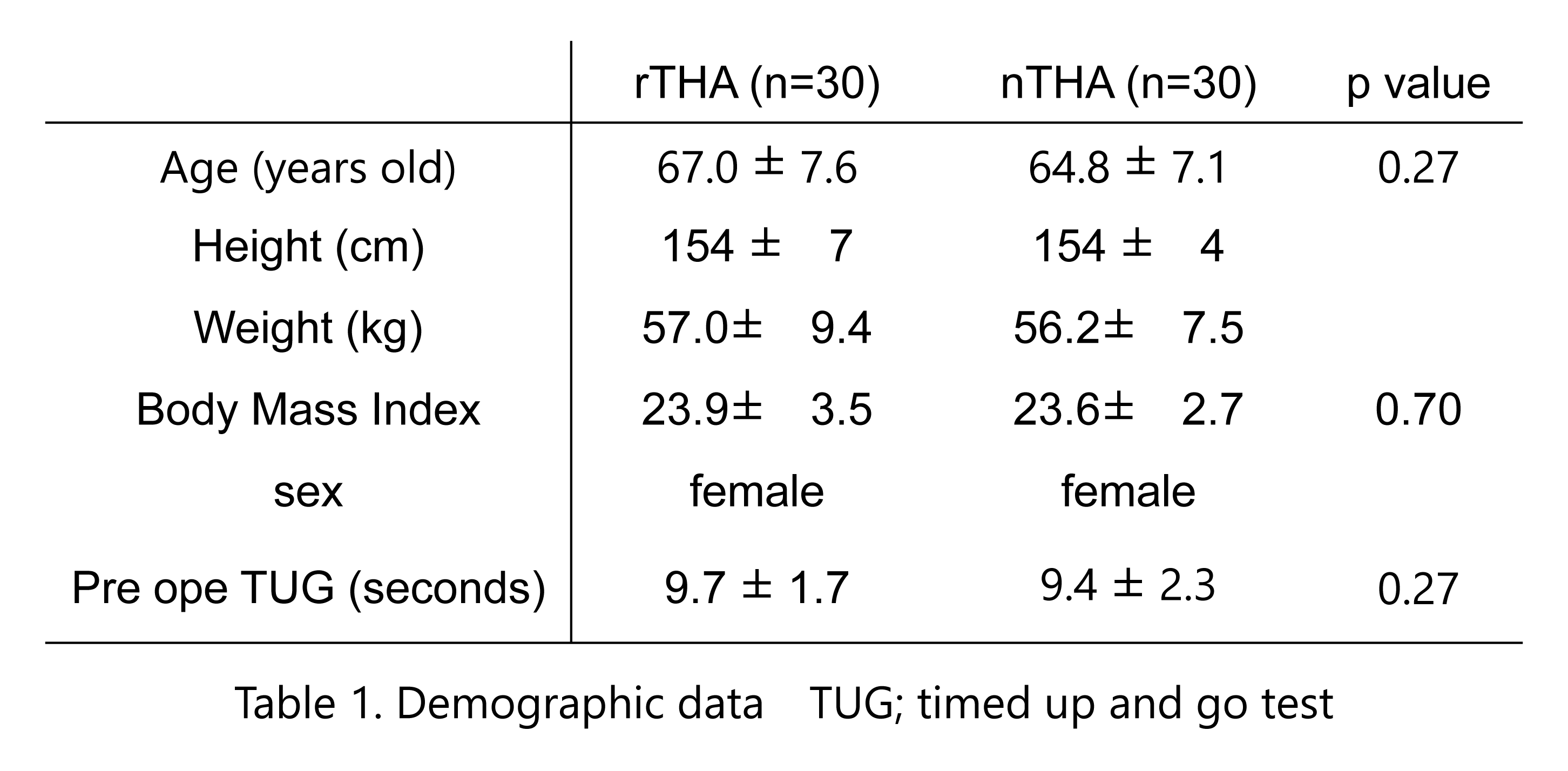
This prospective comparative study was approved by the institutional review board of our institution and informed consent was obtained from each patient. This study utilized data from a prospective total joint arthroplasty database containing demographic, clinical, and radiographic data on all primary THA procedures performed at our institution from February 2018 to January 2020. The clinical and radiographic results of a single senior surgeon at our institution following primary THA were reviewed. After robotic arm-assisted systems (Stryker Mako, Ft. Lauderdale, FL) was covered by insurance in Japan, the surgeon switched from nTHA (Computed Tomography [CT]-based Hip Navigation version 1.1, Stryker Navigation, Freiburg, Germany) to rTHA (Stryker Mako) for all primary THA in June 2019. Among the 70 consecutive THA cases, female patients were selected to exclude the influence of sex on clinical outcome variance. Therefore, this study included 30 cases each of nTHA and rTHA.
Surgical technique
All THAs were performed using the posterolateral approach, with patients in the lateral decubitus position. All hips were implanted with a cementless cup (Trident Acetabular Shell, Stryker Orthopedics, NJ, USA), a cemented stem (Exeter V40 Femoral Stem, Stryker Orthopedics, NJ, USA), ceramic 32-mm head (BIOLOX Delta V40 Ceramic Head, Stryker Orthopedics, NJ, USA), and non-elevated ultra-high-molecular-weight polyethylene liner (Trident X3 insert, Stryker Orthopaedics, NJ, USA). Preoperative CT was performed in all subjects for navigation and robotic arm-assisted systems. The slice thicknesses were 2.5mm for navigation and 0.625 mm for robotic arm-assisted systems. The surgical procedures, including acetabular reaming and cup placement, differed between nTHA and rTHA, as described below.
nTHA
After placement of a 4.0 mm tracker pin and acetabular exposure, surface mapping registration was performed to match the patients’ bony surface to the preoperative CT. Based on the instructions, the inner parts of the acetabulum were avoided for surface mapping. If a difference of >1.0 mm was found between the surface mapping and the preoperative CT, re-registration was performed until the difference met the safe criteria. Thereafter, the surgeons performed acetabular reaming, during which the surgeons could see both anteversion and lateral inclination angles within the navigation monitor and control these angles manually. As the navigation could not visualize the reaming depth, step-by-step reaming of one mm was performed up to one mm smaller than the preoperative plan, from six mm smaller. The anterior, posterior, and medial wall thicknesses were checked in a timely manner to maintain an adequate reaming center and prevent wall collapse. After the reaming, the surgeon determined the target anteversion and lateral inclination angle using navigation and placed the component manually until the rigid fixations were achieved.
rTHA
After placement of a 4.0 mm tracker pin and acetabular exposure, surface mapping registration was performed to match the patients’ bony surface to the preoperative CT. Robotic systems require pointing within the inner parts of the acetabular space. The difference between registration and preoperative CT was 0.5 mm in the rTHA. Single-step reaming a reamer one mm smaller in size was performed with robotic arm-assistance. The MAKO system also guided the component placement angle and depth. If protrusions > three mm were found, same-size reaming was repeated to achieve an adequate depth of fixation. The target inclination and anteversion angles in both groups were 40° and 20°, respectively.
The Mako Total Hip system does not track the stem itself during stem insertion. Thus, in all THAs (nTHA and rTHA), a cemented stem was inserted at the target angle in the femoral canal using a navigation system. The stem anteversion was adjusted to match the anatomical neck anteversion.
The preoperative assessment, patient education program, pain management protocol, and postoperative rehabilitation protocol were the same for both groups throughout the study period.
Evaluations
Patient demographics (age, sex, diagnosis, height, and weight) and clinical data (surgical time, intraoperative blood loss, length of stay in hospital [LOS], pain severity, and the number of days to independent walking) were recorded for both groups. In addition, Harris Hip Score (HHS) was determined preoperatively within one week before surgery and at the discharge. These data were statistically compared between the two groups.
Pain severity
Post-surgical pain severity was evaluated using a numeric rating scale (NRS) for pain, with zero and ten indicating no and worst imaginable pain, respectively. The NRS during motion was evaluated on postoperative days (PODs) one, three, seven, ten, and 14.
Physical function
The number of days to independent walking was defined as the period required for the patient to achieve a defined standard of independent walking using a T-cane. The following conditions had to be met with physical therapists observing the walking: waling for >50 m with a T-cane, patient confidence in their ability to walk with the T-cane, and a timed up and go (TUG) result of <13.5 seconds. The TUG is used to measure the time required to walk a 3.0 m distance, starting and ending with a sitting position. The LOS was recorded as the number of postoperative hospitalization days.
Acetabular component placement, including version and inclination, was assessed radiographically using postoperative anteroposterior (AP) supine X-rays, as previously described [18]. Briefly, the software (Advanced Case Plan Ver2.2; Stryker) created a horizontal reference line along the inferior aspect of the pelvic inter-ischial line as well as a complex of lines comprising a sphere, a concentric ellipse, and a bisecting line bisecting the ellipse along its long axis. While the lines comprising this complex could be manipulated individually, their relationships to each other remained unchanged. The sphere was then manipulated to fit the circumference of the acetabular cup and the ellipse to fit the opening of the cup. The relative ratio of the axes of the ellipse corresponded to the cup version angle. The angle formed by the bisecting line and the inter-ischial reference line indicated the cup inclination angle.
This system could not differentiate between anteversion and retroversion. For version measurement, the cross-table lateral radiographs of all patients were reviewed using the Woo and Morrey [19] technique to ensure that they were anteverted. The radiographic measurements were performed by two observers blinded to the treatment, with the average used for assessment. The accuracy of the MAKO and navigation measurement were 0.1° and 0.1mm, and 0.5° and 1.0mm, respectively. The accuracy of radiographic measurements was 0.1°. The test-retest reliability of the measurements was excellent (interclass and intraclass correlation coefficients, 0.85 – 0.94)
Statistical analysis
Data analyses were performed using a statistical software package (IBM SPSS Statistics for Windows, version 21.0, Armonk, NY, USA). Shapiro–Wilk tests were used to analyze normally distributed data. As the data were normally distributed, the data were expressed as means ± standard deviation (SD). Comparisons between the two independent groups were performed using dependent t-tests. A statistical a priori power analysis was performed using the G*Power software (version 3.1.9.2; Heinrich Heine Universität Düsseldorf, DE) to determine the sample size based on the difference of the days to independent walking between the two groups, using a prespecified significance level of α < 0.05, a power level of 80%, and an effect size based on the results of the pilot study with ten cases (effect size d = 0.70). The estimated sample size was 26 patients in each group, and the post hoc power analysis further confirmed that the power was 0.99. A p-value < 0.05 was set as the level of significance.
{kind=link}