Data source
The study involves a retrospective analysis of claims data from the OptumLabs® Data Warehouse (OLDW), which includes de-identified claims data for privately-insured and Medicare Advantage enrollees in a large, private, U.S. health plan. The database contains longitudinal health information on enrollees, representing a diverse mixture of ages, ethnicities and geographical regions across the United States. The health plan provides comprehensive full insurance coverage for physician, hospital, and prescription drug services.71
All available healthcare costs were measured and adjusted for inflation to 2018 USD, using the medical care component of the Consumer Price Index. Cost data represent amounts paid by the health plan, and was operationalized as a sum of paid expenditures covered by the Data were analyzed using Stata 14/MP (StataCorp, TX, USA). Institutional Review Board (IRB) approval was obtained from the IRB of the University of Maryland, Baltimore, on July 27, 2016 (HP-00068329).
Study design and variables
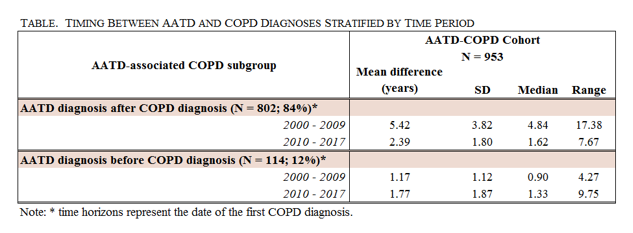
AATD-associated COPD patients were identified based on ≥ 1 diagnosis claim(s) for AATD (ICD-9: 273.4; ICD-10: E88.01) and ≥ 2 diagnosis claims for COPD (emphysema: ICD-9: 492.x, ICD-10: J43.x; chronic bronchitis: ICD-9: 491.x, ICD-10: J40, J41.x, J42.x; bronchiectasis: ICD-9: 494.x, ICD-10: J47; chronic airway obstruction, not elsewhere classified: ICD-9: 496, ICD-10: J44). After AATD-associated COPD patients were excluded from the COPD patient pool, non-Alpha-1-associated COPD cohort was identified based on ≥ 2 diagnosis claims for COPD. The index date was the date of the initial COPD diagnosis claim. Only adult patients at least 30 years of age at the index date were included in the analysis. The time horizon for this study was January 2000 – August 2017. Patients over 65 years of age for whom Medicare was their primary payer were excludedto avoid bias resulting from unobserved costs. At least 12 months of continuous enrollment before and after the index date was required for both cohorts (Figure 1). The cohorts include patients who had medical coverage (with no RX coverage) as well as patients with both medical and RX coverage (for a subset of patients who had RX coverage through the same payer). Only newly diagnosed patients (incident cohort) who did not have COPD diagnoses nor pharmacy claims for COPD medications (identified using National Drug Codes, NDC) 12 months before the index date denoting the washout period were included in the analysis.
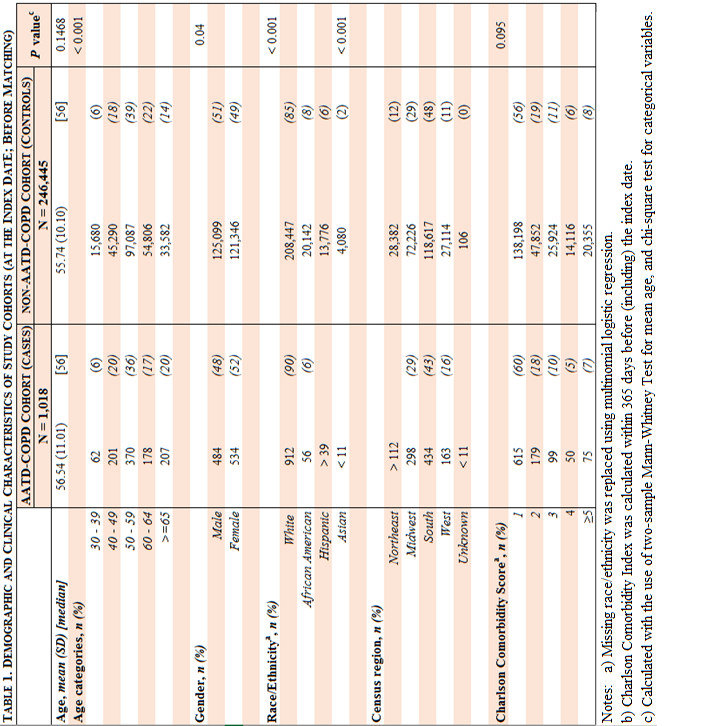
Patient demographics and clinical characteristics collected from enrollment and claims files at the index date included: age, age categories, gender, race/ethnicity, census region and Quan’s Charlson Comorbidity Index (containing both ICD-9-CM and ICD-10-CM diagnoses codes) calculated within 365 days preceding the index date (including index date).72-74 Missing race/ethnicity was imputed using multinomial logistic regression.
Insurers’ costs were calculated and categorized into the following resource categories: all costs (TOT), office visits (OV), outpatient visits (office visits in a hospital setting; OP), emergency room visits (ER), inpatients stays (IP), prescription drugs costs (RX), and other costs (OTH). Costs were defined as amounts paid by insurers’ (third-party payers’ perspective) and measured as all healthcare costs, not COPD-only costs.
AATD-associated COPD patients with ≥ 1 diagnosis claim(s) for AATD were matched with up to 10 unique non-AATD-associated COPD controls. The exact matching algorithm without replacement included the following variables: gender, Quan’s Charlson Comorbidity Score, census region, race/ethnicity, age at diagnosis (+/- 1 year), year of COPD diagnosis and oxygen use (Yes/No; within the first 12 months after the index date) as a proxy for COPD severity.
Multivariate analyses
There were two hypotheses: 1): Patients with AATD utilize more health care resources (incurring higher direct medical costs) as compared to patients without AATD within 12 months before receiving their initial COPD diagnosis. 2) Patients with AATD-associated COPD utilize more health care resources (incurring higher direct medical costs) as compared to patients with non-AATD-associated COPD within 12 months before and after receiving their initial COPD diagnosis.
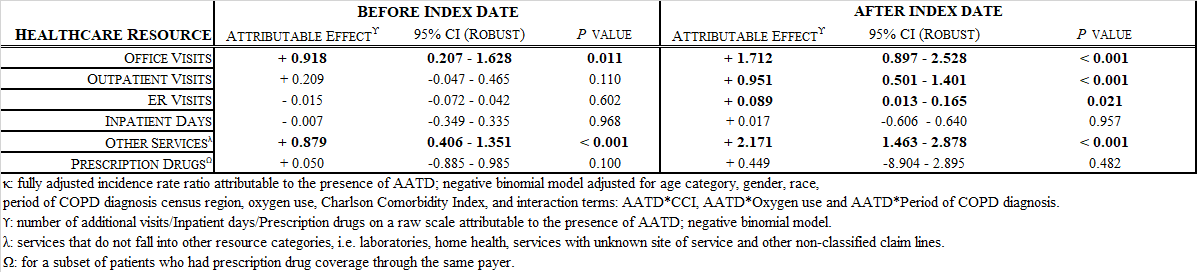
The sum of ER, OV, and OP visits, RX, IP and OTH per patient were modeled in pre- and post-index periods separately using models for count data. Overall, four different count models have been tested: a Poisson, a zero-inflated Poisson, a negative binomial, and zero-inflated negative binomial models.75
The use of a particular count data model was based on the goodness-of-fit criteria. The goodness-of-fit criteria for four models included comparisons of the Akaike’s (AIC) and Bayesian Information Criterion (BIC) for every resource category separately, both before and after the index date.75
To test the hypotheses linked to resource utilization among AATD-associated COPD patients, a dummy variable on the Alpha-1 status for each healthcare resource category before and after index date was investigated for statistical significance (α = 0.05).
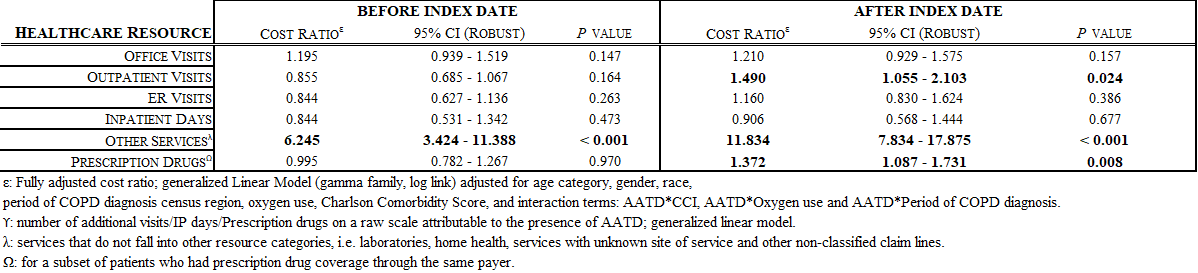
Total 12-month pre- and post-index costs were modeled using a generalized linear model (GLM). In addition, the 12-month pre-and post-index date costs were modeled separately and reported for each resource category.
The choice of the link function and distribution family was conducted sequentially.75 Six different GLMs were compared based on different links and family distributions: log-gamma, square root – gamma, log – Gaussian, square root – Gaussian, log-Poisson, and square-root Poisson model.75
The link test was conducted using the Box-Cox approach, the Pearson Correlation test, the Pregibon link test and the modified Hosmer and Lemeshow test.75
The family distribution was assessed using the modified Park test.75 This test investigates the relationship between the variance of the error term and mean, and the value of the coefficient serves as the guidance for the choice of family distribution.75 Misspecifications test for GLMs were conducted using the RESET test.76
The choice of a final model was based on the goodness-of-fit criteria (the lowest AIC and BIC values) across tested GLM models, as well as the assessment of deviance residuals and a Q-Q plot of deviance residuals.
Adjusted results are presented as ratios of expected costs between both cohorts as well as grand margins. To test the hypotheses, in the GLM model, dummy variable on the Alpha-1 status was investigated for statistical significance (α = 0.05) and then bootstrapped with replacement 1,000 times.
To assess whether a two-stage (hurdle) model should be used, the proportions of patients with total pre- and post-index costs equal to zero were calculated.
Sensitivity analyses
In the one-way sensitivity analysis, the impact of the number of AATD diagnosis claims on costs was investigated: the total cost estimates were re-calculated for AATD-associated COPD patients with ≥ 2 diagnosis claims for AATD to account for the potential of rule-out diagnoses (testing for AATD). In addition, the impact of the 1:10 matching ratio on total pre- and post-index costs was investigated.
In a multi-way sensitivity analysis, both the impact of ≥ 2 AATD diagnosis claims and the 1:10 matching ratio on the total pre-and post-index costs were investigated at the same time.
{kind=link}
{kind=link}
{kind=link}
{kind=link}