In the present study, we examined the clinical significance of preoperative SII to predict postoperative survival outcomes in GC. The optimal cut-off value of preoperative SII for predicting OS was set at 395 according to the ROC curve analysis. The results obtained demonstrated that SII, a combination of three CBC parameters (Neut, Lymp, and Plt), was an independent risk factor for poor OS and RFS as well as pT and pN. Of special note was that high SII correlated with peritoneal recurrence. These results suggested that preoperative SII will contribute to perioperative precise care and adjuvant treatments for patients with GC undergoing curative gastrectomy.
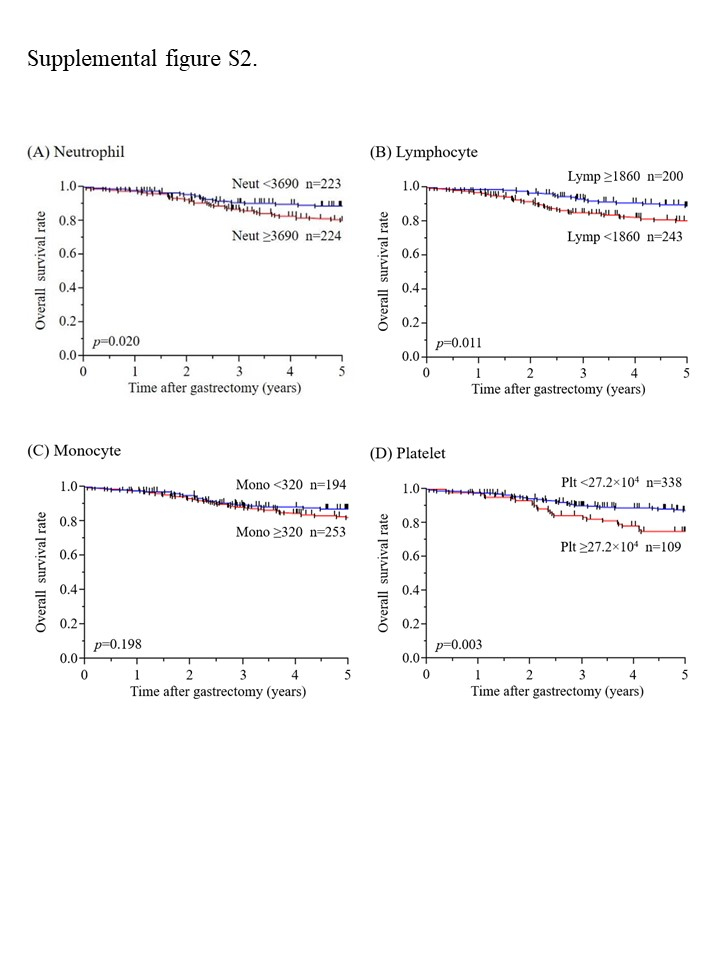
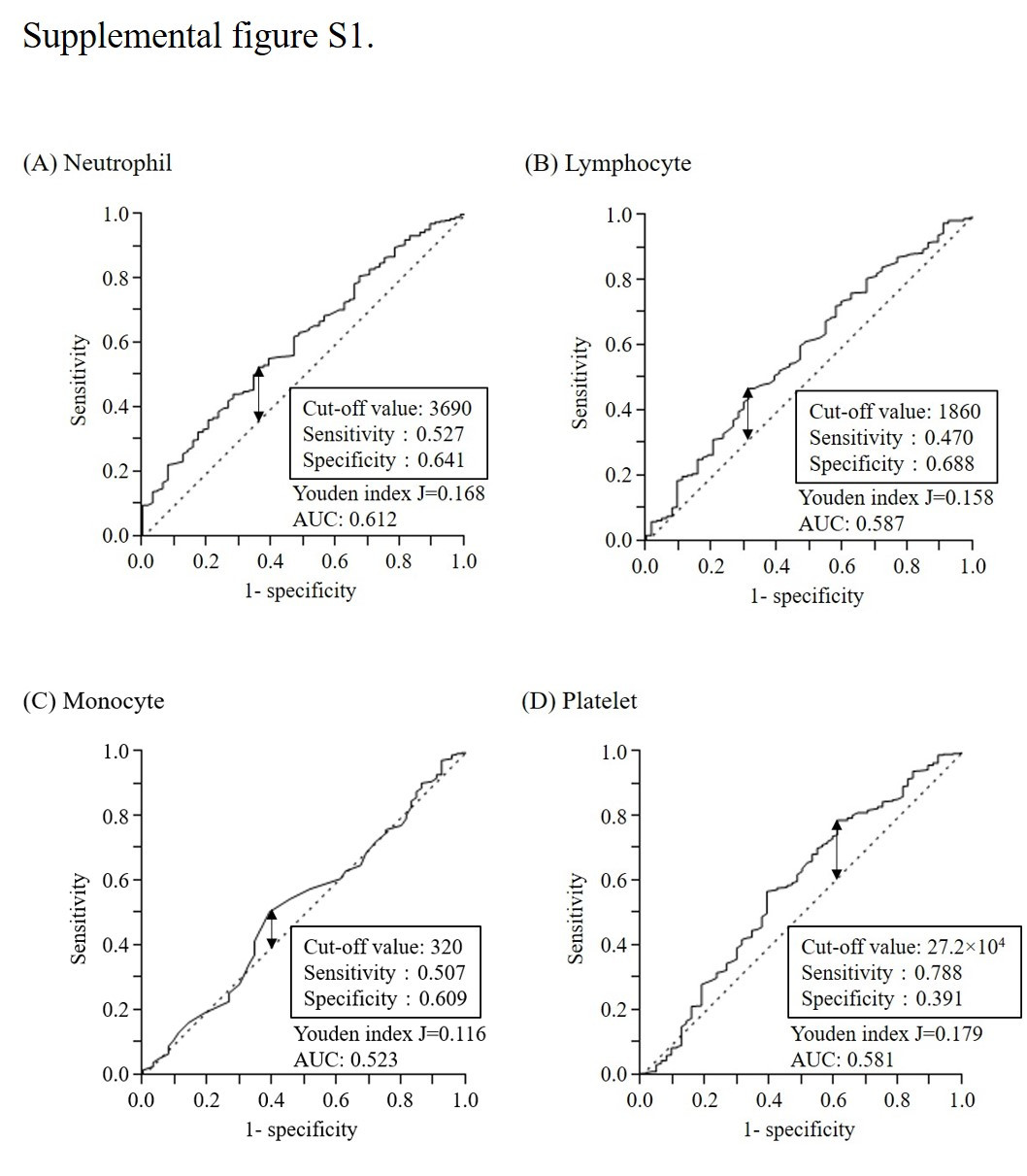
Neutrophilia, lymphopenia, and thrombocytosis each affect a host’s immune-inflammatory status and tumor progression, and have been implicated in poor cancer survival(17–22). Accordingly, high SII, resulting from neutrophilia, lymphopenia, and thrombocytosis, may also be a useful prognostic indicator. In the present study, univariate survival analyses showed that Neut, Lymp, and Plt were significant prognostic factors in patients with GC; however, the multivariate survival analysis (model #1) only identified Neut ≥ 3690 (HR 1.938; 95% CI 1.100-3.488; p = 0.022) as an independent risk factor of poor OS. The multivariate survival analysis (model #2) also identified SII ≥ 395 (HR 3.016; 95% CI 1.593–6.262; p < 0.001) as an independent risk factor of poor OS, with a higher HR and lower p value than those of Neut in model #1. The AUC value showing the predictive power of SII for OS (AUC 0.650) was higher than that (AUC 0.612) of Neut, suggesting that SII, a combination of three CBC parameters (Neut, Lymp, and Plt), was superior to each single parameter as a predictor of survival outcomes in GC.
Previous studies demonstrated the negative impact of high preoperative SII on the survival outcomes of GC(23–25); however, the cut-off values of SII differed between these studies. Wang et al.(23) reported that the optimal cut-off value of SII for predicting OS was 660 (AUC 0.612) according to the ROC curve analysis, and SII ≥ 660 was an independent predictor of OS in GC patients. Hirahara et al.(24) showed that the optimal cut-off value of SII for predicting OS was 661.9 (AUC 0.584) according to the ROC curve analysis, and SII ≥ 661.9 was an independent prognostic indicator in GC patients, particularly in the elderly population. In the present study, although an ROC curve analysis was also used, the optimal cut-off value of SII for predicting OS was 395, which was markedly lower than 600. Nevertheless, the AUC value (AUC 0.650) showing the predictive power of SII for OS in the present study was higher than those of Wang et al. (AUC 0.612) and Hirahara et al. (AUC 0.584); therefore, further studies are needed to validate the optimal cut-off value of SII.
The present study demonstrated that preoperative SII was a risk factor for poor RFS independent of pT and pN, and that SII ≥ 395 correlated with GC recurrence, particularly peritoneal recurrence. To the best of our knowledge, this is the first study to demonstrate the impact of high SII on the specific recurrence pattern of GC. Previous studies indicated that lymphopenia and thrombocytosis were predictive factors for peritoneal dissemination(26, 27). Since high SII results from lymphopenia and thrombocytosis, it may also be a useful predictor of peritoneal recurrence. According to JGCTG, the current indication of postoperative adjuvant chemotherapy is assessed only by pStage (pT and pN). However, the present results suggest that patients with high preoperative SII need to be treated with adjuvant chemotherapy regardless of pT and pN. Furthermore, in patients with high preoperative SII, meticulous postoperative surveillance is crucial for the early detection of GC recurrence, particularly peritoneal recurrence.
The present study had several limitations. It was a retrospective study with a small sample size from one institution, which may have limited its statistical power and generated statistical biases. Furthermore, since the cut-off values of Neut, Lymp, Mono, Plt, and SII were only calculated by a mathematical method, further validations are needed to confirm whether these values are clinically meaningful and applicable to other cohorts. In addition, the present study only examined CBC parameters; however, serum immune-nutritional markers may also be useful predictors of survival outcomes in GC. Nevertheless, the present study clearly demonstrated the novel potential of preoperative SII for predicting postoperative survival outcomes and recurrence patterns in GC over that of each CBC parameter (Neut, Lymp, Mono, and Plt). The results of the present study and the optimal cut-off value of SII need to be validated in further studies with large sample sizes in order to establish a novel perioperative care system according to preoperative SII levels.
{kind=link}
{kind=link}