In this study, we evaluated the eyes with LMH in two subtypes and compared with fellow eyes and healthy controls using OCTA. Our results emphasize superficial microvascular involvement in the degenerative and tractional groups compared to their fellow eyes. Furthermore, superficial, deep and choriocapillaris vascular densities in the LMH groups showed lower values than the control eyes.
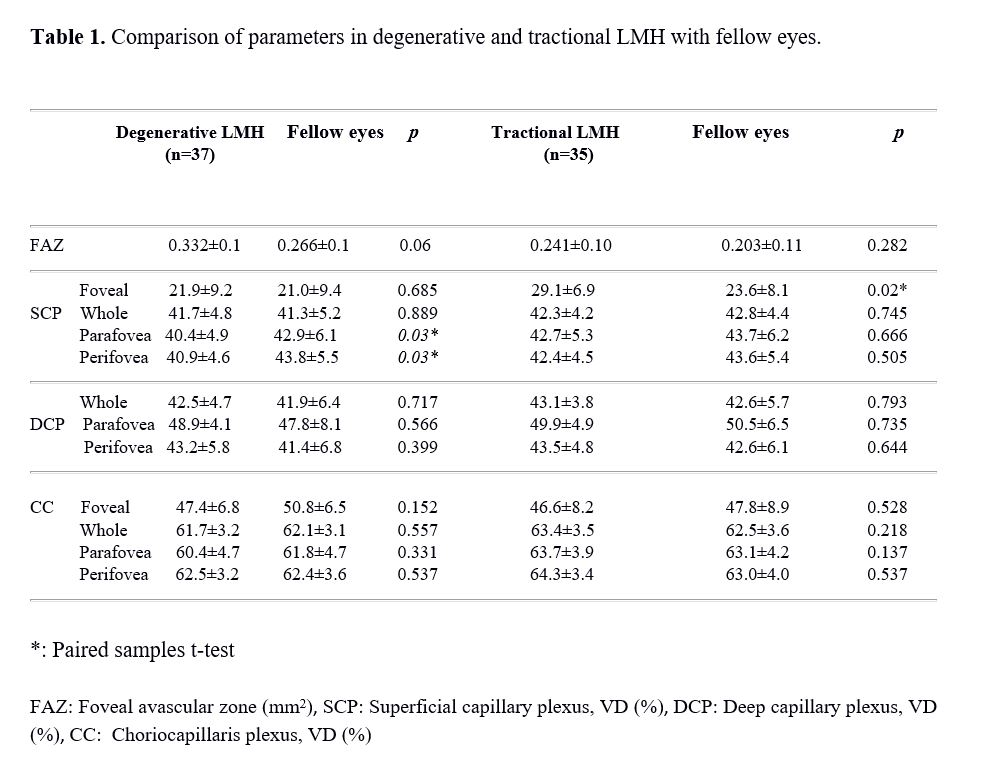
Pierro et al. compared full thickness macular hole, LMH, macular pseudohole and healthy patients using OCTA and revealed vascular engorgement in especially DCP increasingly from LMH to the full thickness macular holes. In their study, they hypothesized that the alterations in SCP and DCP of unaffected fellow eyes may be a sign of early contribution to the development of macular holes 10. Although we did not find any difference between fellow eyes and tractional LMHs apart from the foveal vascular density, a decrease in SCP was found in degenerative LMHs compared to their fellow eyes.
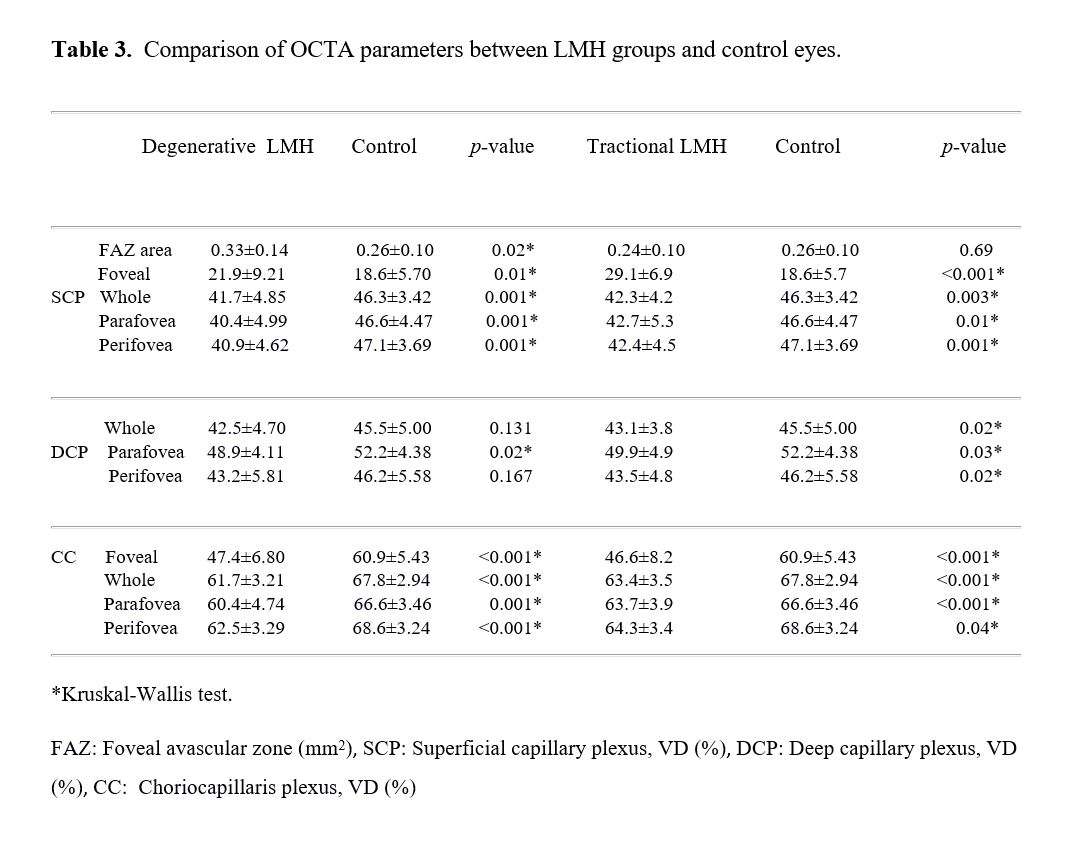
Ahn et al. compared 19 eyes with LMH with normal controls and showed that the choriocapillaris vascular density was not different from the normal control group. They found an association between choriocapillaris flow and outer retinal integrity in full thickness macular hole cases, but not in LMH eyes 12. In our study, decreased vascular densities were found in the superficial and choriocapillaris layers in both degenerative and tractional type LMHs compared to control eyes. In addition, vascular density in the DCP was decreased in the tractional group compared to the control eyes, and a decrease in the parafoveal area of the DCP was observed in the degenerative group. These findings may suggest an association of blood flow variation in the macular degeneration process.
Another study investigating the differences between degenerative LMHs and healthy eyes described a larger FAZ area and higher vascular density in the SCP as compared healthy eyes. Additionally, they found increased vascular density in unaffected fellow eyes 13. We found also larger FAZ area in degenerative group than healthy eyes. The larger FAZ area in the degenerative-subtype may be explained by the involvement of all retinal layers and may be considered a chronic degenerative process.
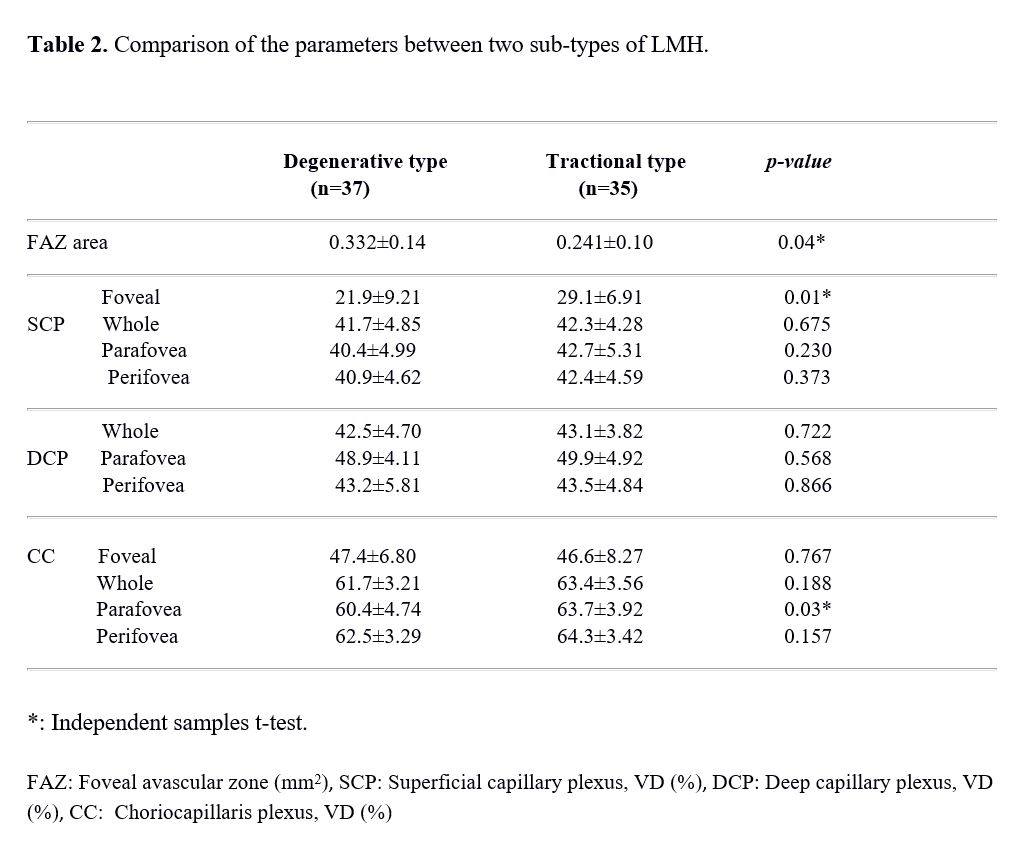
According to Govetto et al., the pathophysiological development mechanisms of the tractional and degenerative subtypes of LMH may differ from each other 14. In the tractional type, there is a schisis-like separation in the outer plexiform and outer nuclear layers secondary to traction, whereas in the degenerative type, there is a slow, chronic separation process involving all layers of the retina 15,16. Also, Kashani et al. have described previously the reversible retinal vascular perfusion alteration due to the direct mechanical effect of vitreous traction in these cases 17. In the present study; the higher foveal vascular density in the tractional type may be explained by the tangential traction. Previous studies have also suggested that tractional forces induce microvascular changes and circulatory disturbances 18,19.
Yeo et al. compared LMH in two subtypes with the control group and found FAZ area and foveal vascular density alterations both in tractional and degenerative subtypes 20. The smaller FAZ area and higher foveal vascular density in the tractional group were similar to our results and was explained by the tangential traction mechanism as in the ERM. They found lower parafoveal vascular densities at the SCP and DCP in the degenerative group than those of the control group. In our comparison, we also found lower vascular densities in the degenerative group compared to the control eyes. On the other hand, the differences between the two subgroups suggest that the formation mechanisms of degenerative and tractional subgroups are different despite their clinical similarities.
The present study has several limitations. We studied a relatively small number of cases. Also, current study did not include patients who had macular surgery for LMH which could change the monitoring for microvascular changes.
Our results suggest that the macula in two subgroups of LMH shows differences in foveal hemodynamics. The different vascular features we determined in two different subtypes of LMH may be due to pathological changes associated with development process. There are limited data to demonstrate the macular capillary plexuses of eyes with LMH in two subtypes using OCTA.
In conclusion, the significant differences we revealed in the retinal microvasculature in degenerative and tractional LMHs may shed light on pathophysiologic mechanism. Also, these parameters may be used as a biomarker for disease progression. These results support the hypothesis of two distinct pathogenic formation for different subtypes. Larger studies observing retinal microvascularization and the alterations will further contribute to our clinical approach.
{kind=link}
{kind=link}
{kind=link}