The medical student participants provided unprompted examples of humour from their experiences of communication in clinical settings. Specifically, participants provided accounts of a potentially problematic humour use: a kind of tendentious or superiority humour that is aberrant, or humour that departs from an acceptable standard. Notably, participants did not outline any examples of potentially non-problematic humour e.g. incongruity humour use, with only one example of Self Disparaging Humour (a sub category of Superiority Humour) being used as an alignment strategy. We now review three examples of ‘aberrant humour’.
Aberrant Humour: 1 – The elevator (surgeon)
The following is an abbreviated account of problematic humour that took place frontstage in a lift in X hospital. Present was a male surgeon, a junior doctor (female mentor), 3 male/female medical students and 2 others e.g. patients or relatives.
“He (the surgeon) saw me writing notes and he says, “Oh what are you writing?”
I don’t know this Doctor I have never seen him, I said that I am just writing patients notes and he just takes the note book out of my hand and starts reading my notes out loud in the lift and he’s laughing, he’s going ‘oh [laughter] or why did you write this?’ [laughter]. I have never experienced anything like this.
He read [aloud] what I had written on the page, handed the book back to me and left, and he was laughing the entire time.
I didn’t know what to do [laughter]. I was laughing because I didn’t know how to handle it..
He (the surgeon) was laughing, so you have to laugh….
1:B: 11-372
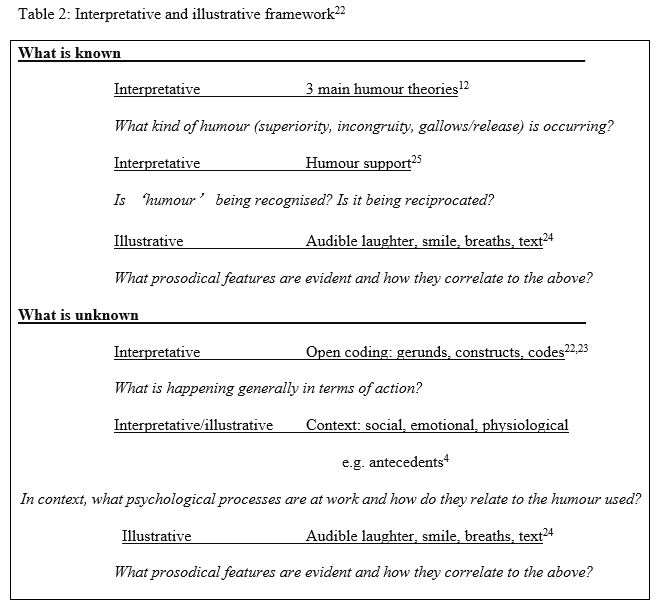
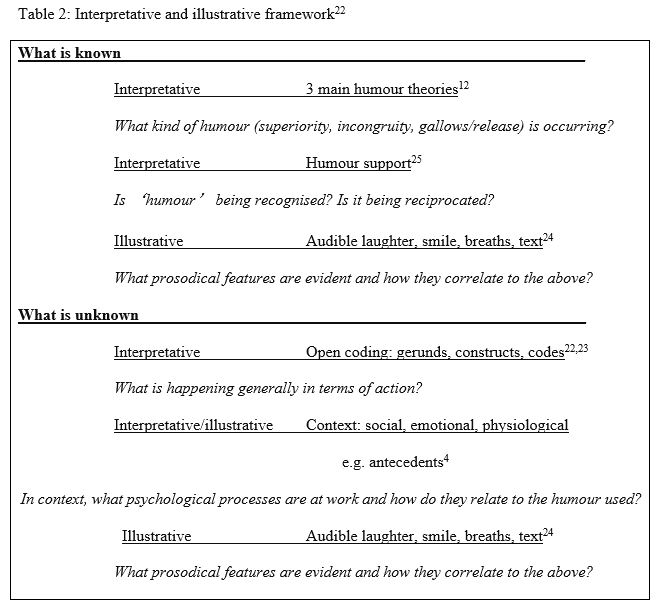
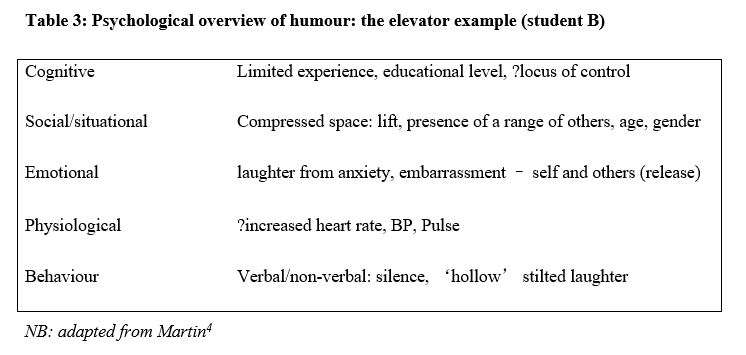
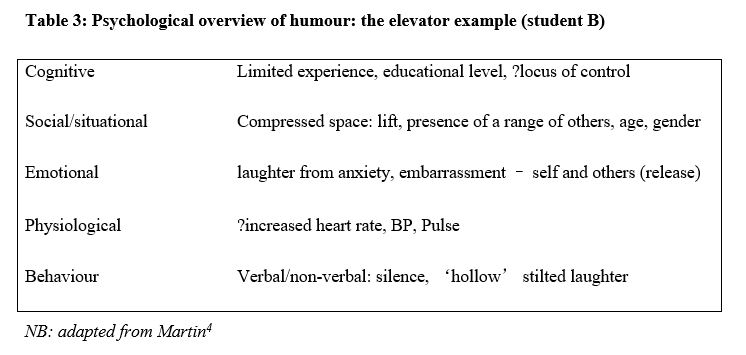
The above account is an example of problematic tendentious humour presumably aimed at ridiculing the student in question in front of a mixed audience in a public place. The student reported initially resisting the surgeon’s attempts to acquire the notebook but then acquiesced. Student B then highlights her confusion at this behaviour by (self-disparagement) laughter here but reports expressing release laughter at the time. She states later she sensed others in the lift were similarly confused and embarrassed and when pressed for more information on the laughter sequences, recounts that initial silence gave way to stilted laughter particles and then more sustained laughter particles which concluded when the surgeon stopped reading and exited the lift.
According to Hay’s25 humour support strategies, humour in the above sequence is recognised but not understood, appreciated nor necessarily agreed and is therefore, not wholly supported. Rather, student B eventually concurred that she laughed due to a potential myriad of reasons e.g. (a) release through her perceived embarrassment (b) confusion (c) to reduce the perceived awkwardness/embarrassment of others in the lift (d) because he (the surgeon) was trying to be funny, (e) he was a clinical ‘superior’ and (f) to simply get him to stop reading. Thus, the student unwittingly perhaps, provides a psychological overview of the situation (table 3) which is not as simple as it may initially appear. There is reciprocal laughter but only as an appeasement strategy to bring the problematic humour expression to a quick end for all. Prepositions that normally follow the verb ‘laugh’ are mainly to laugh (a) at, (b) about or (c) with. However, in this example the appropriate preposition is arguably ‘for’: not indicating a time period but someone, in this case a superior who is patently showboating at the unfortunate student’s expense.
A number of medical students reported similarly embarrassing episodes of superiority humour aimed at ridiculing medical peers in front of a group. However, these episodes appeared to be exclusive to one specific hospital known which evidenced outdated medical hierarchies or approaches. Students patently recognised this as aberrant humour use albeit their cognitive appreciation was somewhat under-developed. A greater understanding of the (humour) processes taking place may have helped them to respond differently and to have been better able to cope with any potential impact upon their sense of self, especially if exposed to repeated episodes.
Aberrant Humour 2: ‘He’s dead’ (Psychiatrist)
The following example in the same hospital is one of potentially aberrant humour that was not viewed as such by the students providing the account. In this account, the student recalls a patient knocking at an open door, asking for a particular doctor. The consultant looks at the patient and states; ‘Oh he’s dead (giggling laughter)’ – to which the patient replies he has an appointment. ‘No can do’says the consultant
2:477:C
‘We (medical students) get a kick out of it, he (the consultant) gets a kick out of it and then he explains to the patient where to go’…….he wasn’t making fun of.. or with the patient.. he was making a joke of the patients’ request but then proceeded to answer the request eventually.
2:487:C
The prevailing view therefore, appeared to be this was harmless recreational humour for the students’ benefit to promote inclusion (‘this one’s for you guys’) and no harm accrued as the patient was appropriately re-directed. Notably, some of the non-Arab speaking medical student participants reported feeling excluded at times particularly in hospital X. Consequently, when a consultant made an effort to include them in humour they might understandably find this gratifyingly inclusive with superiority humour having the potential to promote group inclusion27 Nevertheless, some participants were perhaps unable to distinguish inappropriate/aberrant humour being used as potentially distracting, recreational, ridiculing or perhaps, as simply individual relief at not being the butt of the joke.
Aberrant Humour 3: hu::ge balloon (Psychiatrist)
The final example is a patient who was attending the same consultant in example two following ‘a bleed in her brain’ which had resulted in a series of psychiatric symptoms:
He was trying to explain the reason behind getting this bleeding in her brain, and he was like… listen to me, in a very sarcastic way in a very thick accent in X, he was like “listen, you have this kind of ve::ry ve::ry very hu::ge balloon”
2:508:A
The student reporting the example drew laughter from the rest of the focus group and then stated that the patient had reproached the Doctor - “Stop being sarcastic doctor, I’m tired” – before, she too started to laugh. The student was asked about the import of humour in this example and its appropriateness or otherwise in this situation:
Maybe it’s a way for him to distract the patient from their own zone to get them out of the depression and the anxiety mood.
2:520:A
(At the) end of the day he treats anxiety and this should be managed by a neurologist..
2:526:A
You know, so if it’s not well explained for her it’s not his job because he is a psychiatrist not a neurologist.
2:530:A
Thus, student A – who drew agreement from her fellow participants – considered the humour used in this situation to be recreational and distracting i.e. a positive emotion, while Chung et al28 notes that medical students are empathetic to their clinical trainers irrespective of possible aberrant behaviour. However, the student’s assertion that the surgery and outcome was not the province of the psychiatrist and this therefore, fully justified the sarcastic explanation provided was at best tenuous.
{kind=link}
{kind=link}
{kind=link}
{kind=link}