Patient disposition and baseline characteristics
In total, 81 patients with advanced solid tumors were enrolled in the study between August 1, 2018 and May 13, 2021. Patient demographics and baseline characteristics of the study population are summarized in Table 1. Breast, colorectal, and gastric or gastroesophageal junction cancers were present in 90.1% (73/81), 7.4% (6/81), and 2.5% (2/81) of patients. HER2 expression was available for all 81 patients: 64.2% (52/81) were immunohistochemistry (IHC) 3+, 24.7% (20/81) were IHC 2+ and FISH positive, 2.5% (2/81) were IHC2+ but FISH negative, and 8.6% (7/81) were IHC 1+.
The dose escalation set included 22 patients: one at 0.1 mg/kg and three at each of 0.3, 0.6, 1.2, 2.4, 3.6, 4.8, and 6.0 mg/kg dose levels. The dose expansion set included 59 patients: 24 at 4.8 mg/kg and 35 at 6.0 mg/kg. All 81 patients were evaluable for toxicity analysis, whereas 80 were evaluable for tumor response. At the time of the data analysis on July 13, 2022, A166 treatment was discontinued for 68 (84.0%) of the 81 patients, most commonly due to progressive disease in 62 patients, treatment-related AEs (TRAEs) in 5 patients, and protocol deviation in 1 patient.
In total 81 patients, 90.1% (73/81) had received at least 3 prior lines of systemic therapy in the metastatic setting. For 66 HER2-positive (IHC 2+ and FISH+, or IHC 3+) breast cancer patients, all had prior HER2-targeted therapy with the median prior line of 4, including 100% (66/66) received trastuzumab ± pertuzumab, 89.4% (59/66) received anti-HER2 TKIs, and 25.8% (17/66) received anti-HER2 ADCs in which 11 received T-DM1, 5 received ARX-788,11 and 1 received TAA013.
Safety
All 81 patients received at least one dose of A166 and were included in the safety analysis. No DLTs were observed in the dose escalation part, thus, the maximum tolerated dose (MTD) was not reached. TRAEs of any grade were documented in 98.8% (80/81) patients (Table 2). Across all dose levels, the most frequent TRAEs of any grade were corneal epitheliopathy (84.0%), blurred vision (74.1%), peripheral sensory neuropathy (53.1%), dry eyes (32.1%), muscular weakness (28.4%), anemia (23.5%), blood creatine phosphokinase increased (22.2%), alopecia (22.2%), alanine aminotransferase (ALT) increased (18.5%), aspartate aminotransferase (AST) increased (18.5%), myoglobin blood increased (17.3%), hyponatraemia (16.0%), and hypomagnesemia (16.0%) (Table 2). TRAEs grading ≥ 3 occurred in 40 patients (49.4%) and included corneal epitheliopathy (30.9%), blurred vision (18.5%), dry eyes (7.4%), peripheral sensory neuropathy (6.2%), anemia (2.5%), hyponatraemia (2.5%), muscular weakness (2.5%), and leucopenia (1.2%).
SAEs related to treatment were reported in four patients (thrombosis [n=1], muscular weakness [n=1], and peripheral sensory neuropathy [n=2]). Only one death occurred during the treatment, which was attributed to progressive disease. TRAEs led to dose reduction and treatment discontinuation in 30.9% (25/81) and 6.2% (5/81) patients, respectively.
PK characteristics
Compared with the 81 patient data set, the PK analysis included 80 patients, one participant at dose of 0.1 mg/kg was excluded due to lack of PK data. Serum concentration–time profiles for A166 ADC in cycle 1–5 at different dose cohorts are shown in Figure 1A. Pharmacokinetic analysis of serum concentrations revealed that the exposure of A166 ADC were increased with each increasing dose level, and did not exhibit dose accumulation at 0.3–1.2 mg/kg, while this ADC had a limited accumulation at 2.4–6.0 mg/kg. At the recommended doses for expansion part (4.8 and 6.0 mg/kg), the accumulation ratio of Cmax was around 1.46-1.51, and area under curve (AUC) was around 1.97-2.15 of A166 ADC, respectively (Table S1). The PK parameters of A166 ADC, TA and Duo-5 for each dose cohort over cycle 1 are summarized in Table S1. Overall, low concentrations of free Duo-5 were observed and the PK characteristics of TA were similar to A166 ADC after administration of A166. At 4.8 and 6.0 mg/kg, the t1/2 of A166 ADC was 8.83 and 8.33 days after the first dose of A166, respectively. The Cmax and AUC of Duo-5 were about 0.1% and 0.2% of the total A166 ADC, respectively (Figure 1B).
In this study, anti-A166 antibody was detected in 12 (14.8%) of 81 patients, 10 of whom were antibody positive at pre-dose, due to prior trastuzumab treatment. The remaining two patients were tested positive in cycle 2 (before dosing) and 6 (before dosing). However, there were no differences in exposure, safety or efficacy of A166 ADC in antibody-positive patients compared to the negative ones.
Efficacy
In total, 80 patients were available for efficacy assessment, one patient from 4.8 mg/kg group was not evaluated because of rapid deterioration of general condition. An objective partial tumor response was observed in 43 patients. A166 showed activity at 3.6 mg/kg, and a dose-response effect was observed with more partial responses in patients treated at 4.8 mg/kg or higher. The doses of 4.8 mg/kg and 6.0 mg/kg A166 were chosen for further investigation in the dose expansion part. At the time of the data cutoff, the median treatment duration was 6.3 months (range, 1.4-34.3) in 4.8 mg/kg cohort and 5.4 months (range, 1.4-23.3) in 6.0 mg/kg cohort, and the median duration of follow-up was 20.3 months (range, 1.9-34.4) in 4.8 mg/kg cohort and 14.8 months (range, 3.1-28.4) in 6.0 mg/kg cohort.
In this phase I trial, for 58 HER2-positive breast cancer patients treated at 4.8 or 6.0 mg/kg (Table 3), ORR was 70.7% (41/58, 95% CI, 57.3–81.9) and DCR was 81.0% (47/58, 95% CI, 68.6–90.1). The waterfall, swimmer, and spider plots of tumor burden alteration over time for each patient are shown in Figures 2A, 2B, and 2C, respectively. Seventeen of 23 patients (17/23, 73.9%, 95% CI, 51.6-89.8) achieved a response in 4.8 mg/kg cohort, whereas 24 of 35 patients (24/35, 68.6%, 95% CI, 50.7-83.2) achieved a response in 6.0 mg/kg cohort. Median PFS was 12.3 months (95% CI, 6.0–not reached) in 4.8 mg/kg cohort and 9.4 months (95% CI, 4.0-10.4) in 6.0 mg/kg cohort.
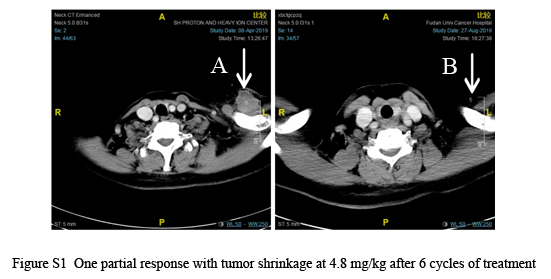
Among patients who showed a response, one patient (4.8 mg/kg) with a diagnosis of hormone receptor-negative, HER2-positive breast cancer and lymph node metastasis showed a duration of response lasting approximately 2 years, and the treatment is still continuing. After six cycles of therapy, the CT scan revealed that the target lesion completely disappeared (Figure S1).
{kind=link}