Demographics
Of the 550 questionnaires that were distributed to participating pediatricians, 452 (response rate, 82%) were completed and analyzed. Thirteen questionnaires were excluded because of missing or incomplete data. Most of the respondents were less than 30 years of age (43.4%), followed by those who were between 30–40 years of age (41.4%), those who were between 41–50 years old (7.1%), and those who were over 50 years of age (8.2%). Our sample had equal female and male respondents 226 (50.0%). Among them, 44% were PRs, 23.7% were PCs, 19.0% were PSs, and 3.1% were PGs. Respondents from government hospitals represented the highest proportion (89.6%), followed by respondents from private hospitals (10.4%). Demographics and practice characteristics of the study participants are presented in Table 1.
Definition, Indication, and Management of Probiotics
When survey respondents were asked about the definition of probiotics, 261 of 452 respondents (57.7%) were aware of the definition of probiotics as live microorganisms, compared with when administered in adequate amounts, confer a health benefit to the host (Figure 1). Among them, 62.8% of PRs and 48.8% of PSs reported that they have little knowledge of probiotics. However, consultants of pediatrics exhibited little knowledge of probiotics (47.7%), while PGs showed that they have excellent knowledge regarding probiotics (42.9%; P<0.001). Correlation between responders’ status and knowledge about probiotics is shown in Table 2.
There were significant differences in the percentage of participants who asked on which systems they think probiotics have an effect. Additionally, 86% of PCs reported that probiotics have effects on the GI system (P<0.001). Assistant consultants (48.4%), associate consultants (40%), PRs (81%), and PSs (68.6%) reported that probiotics have effects on the GI system.
In response to questions about clinical indications for prescribing probiotics, there were no significant differences (P=0.298) between them groups. However, most participants reported that probiotics were used to improve digestion and GI immunity. Correlation between responders’ status and indications of probiotics is shown (Table 3). Among the participants who responded to the survey, most PRs and PSs correctly reported that probiotics reduce the risk of antibiotic-induced diarrhea (74.9% and 80.2%) respectively, but there were no significant differences among them.
When survey respondents were asked about the prescription of probiotics, nearly half of the participants (57.7%) reported that probiotics must be taken before meals. Among them, 61.3% of PRs, 58.9% of PCs, and 57.1% PGs chose the correct answer, but there were no significant differences among them (P=0.182). Association between responders’ status and knowledge of probiotics is shown (Table 4).
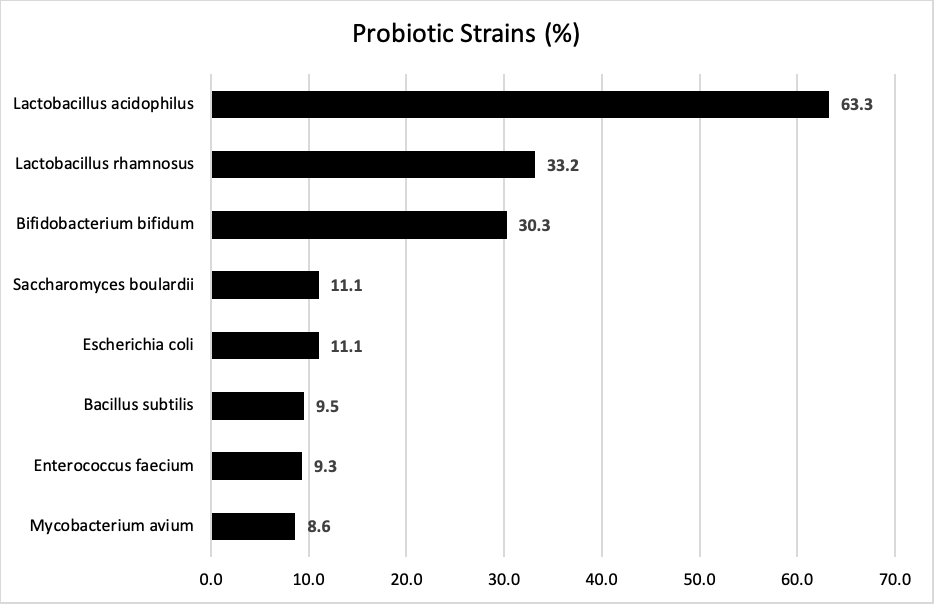
The most common probiotic used by all participants was Lactobacillus acidophilus (63.3%), and Mycobacterium avium was the probiotic least often prescribed (8.6%). The lists of common probiotic strains prescribed were shown (Figure 2). There was no significant difference in Lactobacillus rhamnosus as probiotic strain that was used by pediatricians (P=0.840). Correlation between the responders’ status and knowledge of probiotics is shown (Tables 3, 4).
Regarding the source of probiotics-related information, our study showed that the sources of pediatricians’ information on probiotics included the internet (50.0%), medical journals (44.0%), medical conferences (28.8%), newsletters (11.9%), and radio or TV (8.0%).
In summary, an unanticipated finding of this study was the possible differences in probiotic use practice patterns among PS, PR, PG, ACP, and CP. Overall, the responses indicated that PR and CP were more likely to report themselves as familiar with the literature related to probiotics and the various available probiotic preparations.
{kind=link}