Among complications associated with hemophilia, joint bleeding (hemarthrosis) and subsequent chronic synovitis are the most prevalent, accounting for 65% to 80% of all bleedings in patients with severe hemophilia. [1] Synovitis results from the presence of iron in the joint space that, when interacting with synoviocytes, stimulates the expression of the c-myc and MDM2 proto-oncogenes. These proto-oncogenes allow proliferation of synovial cells and block the apoptotic signaling cascade, ultimately provoking synovial hyperplasia. Simultaneously, macrophages and monocytes migrate to the joint, with secretion of vascular endothelial grow factor, interleukin 1 alpha, interleukin 6 and tumor necrosis factor alpha. These factors are responsible for stimulating osteoclasts, fibroblasts and T cells to produce substances that will promote the proliferation of blood vessels in the synovium and proinflammatory substances that will induce damage to the cartilage and its subsequent degeneration [13–15].]
Synovial hyperplasia is characterized by a rich vasculature and fragility for ruptures due to mild trauma. This will produce a new hemarthrosis that will perpetuate the damage and degeneration of the joint.
Hematologic prophylaxis is recommended as a mechanism for preventing bleedings and preserving normal musculoskeletal function in patients with hemophilia. However, if chronic synovits is already present, despite the use of prophylaxis, synoviorthesis, whether chemical or with radionuclides, should be used [4,9].
The RS was first described by Fellinger Schmid in 1952 as a therapeutic strategy in chronic synovitis, but Ahlberg was the first to use radionuclides for fibrous synovium in patients with hemophilia in 1971 [6].
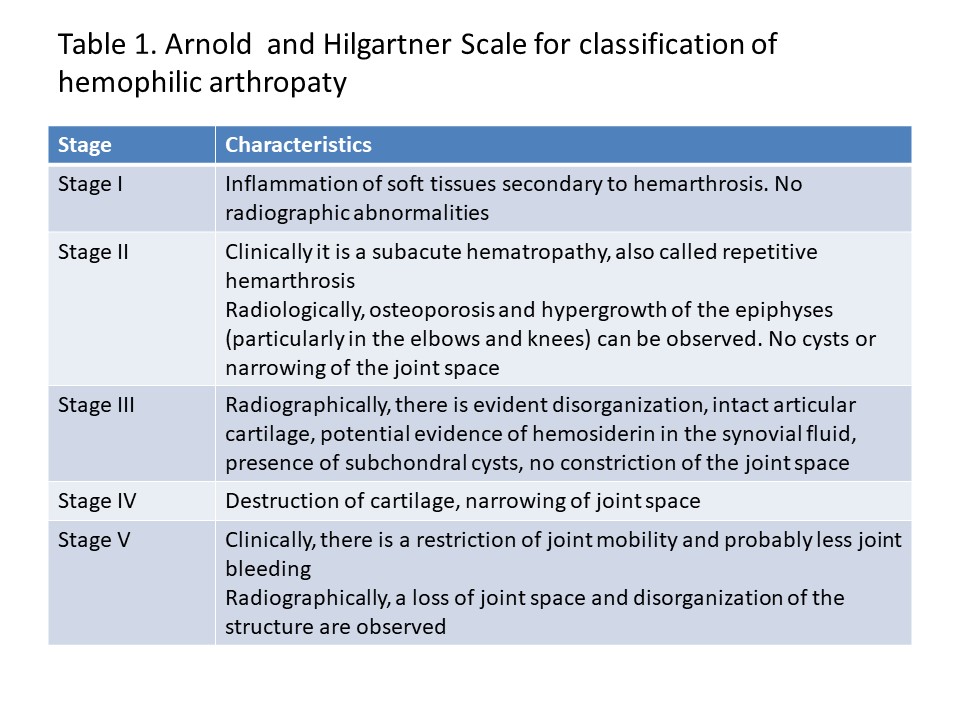
This procedure should be performed after the finding of radiological signs of chronic arthropathy, as well as in grades I-II according the classification proposed by Fernández-Palazzi [4].
Radiographic studies show that, at the tissue level, colloidal suspension is phagocytosed by the macrophages in the superficial layer of the synovial membrane, achieving, with selective irradiation, initial hyperemia and increased leukocyte migration, with subsequent increase of the cellular and humoral defense reaction. The final consequence is a reduction of inflammation. Later, at two or three months, sclerosis and fibrosis of the synovial membrane can be observed [16].
RS in children is a controversial therapeutic procedure due to the use of radioactive isotopes. However, in line with our results, several studies have shown an excellent response to SR in children with hemophilia, and a good safety profile.
Research by Rodríguez-Merchán et al. in the hemophilia center of the Hospital de la Paz in Madrid, Spain, showed an improvement in joint function in young patients treated with RS in whom synovial membranes were not yet severely injured [17]. Heim et al. reported that RS in hemophiliac patients with chronic synovitis provides an 80% decrease in hemarthrosis and that 15% of cases did not present new episodes [18]. Manco-Johnson et al. in a study with 91 joints of 59 children with hemophilia with and without inhibitors of coagulation factors VIII and IX, found that RS limited the frequency of hemarthros, decreased pain, and improved joint function [19]. Kavakli et al in a series of 221 RS in 150 children and young adults reported a reduction of hemarthros in all patients, especially those with grade II synovitis and with early experience with 90Y [20]. Alioglu et al evidenced that RS was the best therapeutic procedure to halt the evolution of chronic hemophiliac synovitis into hemophilic arthropathy in 18 patients with a mean age of 12 years and severe hemophilia with grade I or II synovitis [21]. Also Turkmen et al. in their study on the use of RS with 90Y on 82 knees of 67 pediatric patients and young adults with synovitis secondary to hemophilia showed that it was possible to delay the progression of arthropathy and increase the time to rebleeding [22]. Martínez-Esteve et al. in their series of 20 children and adolescents with hemophilia (mean age 13 years) reported that in the 70.3% of the joints the RS had a good or excellent response and in 29.7% a partial response [23].
The efficacy of RS ranges between 76% and 80%, and the percentage of failure of the procedure in the control of hemarthrosis is considered to be 20%. When compared with chemical synoviorthesis, authors such as Bessant et al. report a variable and changing response throughout the months of evolution, with efficacy being 67% at six months and 50% at twelve months [24].
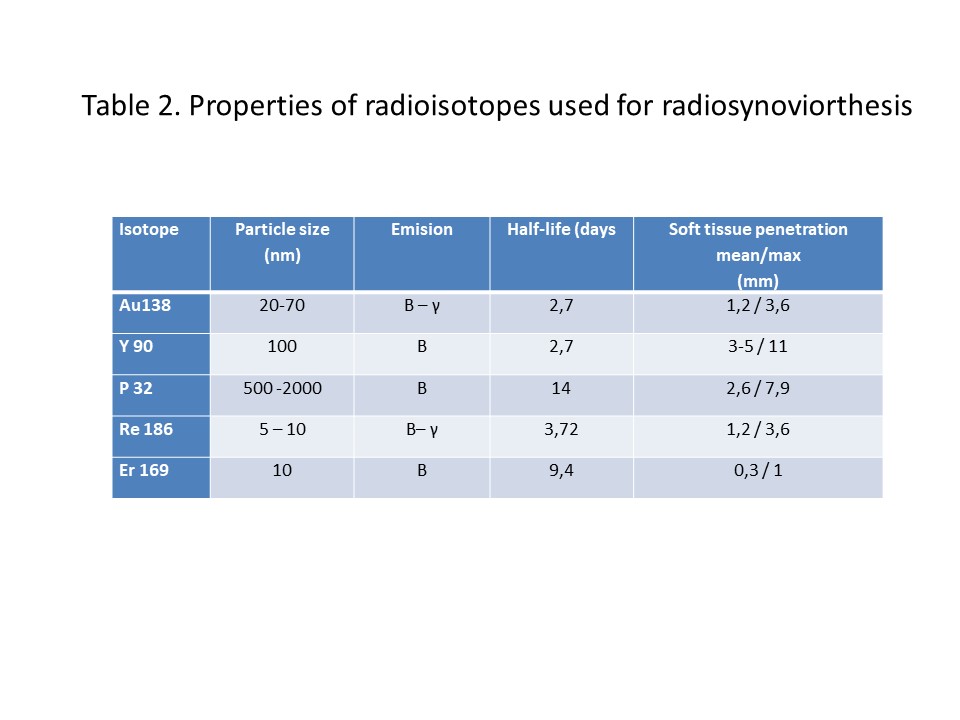
Complications are rare if the technique is performed properly. General complications include fever or allergy to the radiotracer (very rare), and local complications, related to joint puncture, include local pain, septic arthritis or lymphedema. Cutaneous necrosis with fistulization through the needle path is very rare. There is a risk of acute synovitis after treatment, although this possibility decreases when corticosteroids are associated [15]. Premalignant lesions or changes in the structure of chromosomes have not been demonstrated in patients who have been given 90Y and 186 Re [15,25]. In our series, no adverse effects associated with RS were observed.
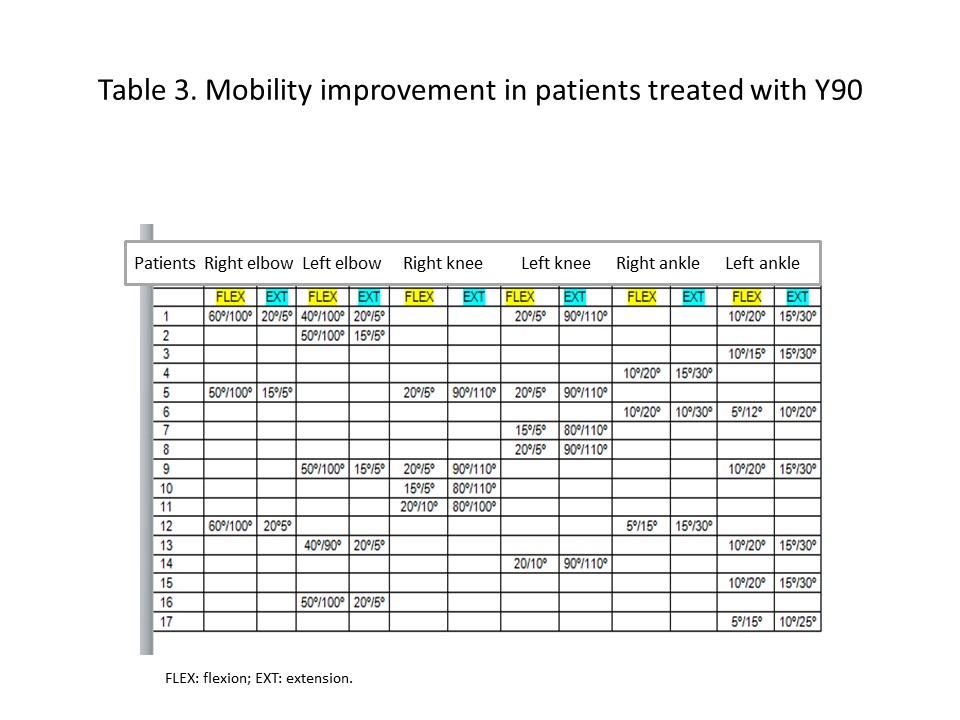
The effectiveness of RS, the decreased number of procedures required for controlling hemarthrosis, the improvement in joint mobility and the lower amount of prophylaxis required are parameters that all together have led to recommend RS as the procedure of choice in patients with haemophilic arthropathy [15].
RS presents a number of advantages such as: simplicity, safety, shorter or unnecessary hospitalization, limited cost, as well as the possibility of repeating the technique without loss of efficacy and performing posterior surgical synovectomy, if necessary [18–23,26].
{kind=link}
{kind=link}
{kind=link}